Successful Reirradiation of Multiply Recurrent Lymphocytic Hypophysitis: A Case Report
Applied Radiation Oncology
Published: April 1, 2026
1 Elliot Regional Cancer Center, Manchester, NH
2 Department of Radiation Oncology, Taussig Cancer Center, Cleveland Clinic Foundation, Cleveland, OH
* Corresponding author: John Suh (suhj@ccf.org)
Abstract
Keywords
Lymphocytic hypophysitis, pituitary dysfunction
Case Summary
The patient originally came to medical attention roughly 6 years prior to his initial course of radiation therapy (RT) after months of progressively worsening headaches. Further workup revealed pan-hypopituitarism and diabetes insipidus. An MRI of the brain demonstrated enlargement, thickening, and enhancement of the pituitary stalk and gland. Systemic staging scans were negative for signs of malignancy. He was started on prednisone (30 mg daily) and azathioprine for presumed neuro-sarcoidosis (azathioprine was eventually stopped after a hospitalization for bacterial meningitis). Ultimately, the decision was made to observe the patient with serial MRI scans while continuing corticosteroids. A few years later, the patient developed bitemporal hemianopsia and associated progression on surveillance imaging. An endoscopic trans-nasal biopsy revealed evidence of chronic inflammation consistent with lymphocytic hypophysitis. He continued steroids, which were eventually tapered to lower doses due to side effects, including steroid-induced diabetes.
Shortly thereafter, he experienced progressive visual changes that correlated with continued inflammatory progression involving the pituitary apparatus and floor of the third ventricle. Progression continued following the start of rituximab. Eventually, he underwent a subtotal resection, resulting in short-term improvement. With continued observation, the patient’s imaging remained stable for the next 2 years.
Imaging Findings
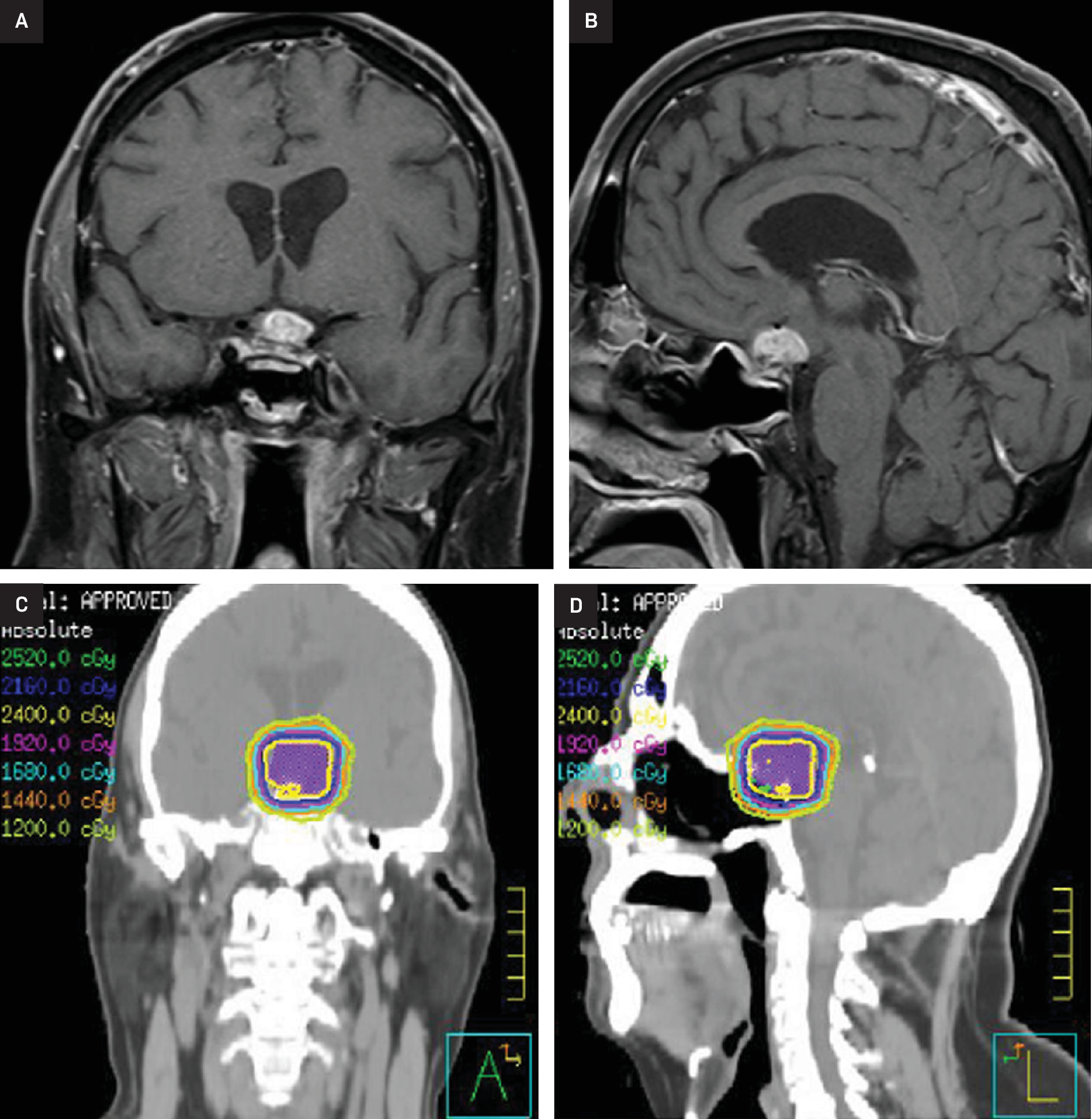
After 2 years of stability, imaging revealed further progression with mass-like enhancement involving the suprasellar cistern, optic apparatus, and hypothalamus, associated with worsening vision. The patient’s case was discussed at multidisciplinary tumor board with the recommendation for radiation. He then received 24 Gy in 12 fractions with 6 MV photons utilizing 2 non-coplanar VMAT arcs and cone-beam CT for image guidance (Figure 1). Areas of progression and enhancement were targeted, including the sella, optic nerves and chiasm, and hypothalamus. He experienced no immediate side effects except for mild fatigue. Within 6 months of his initial course of RT, his vision had improved. At 3 years post RT, he had stable vision with very slight progression on imaging and remained on low-dose steroids. However, by 6 years after RT, the patient’s suprasellar lesion had notably enlarged with an increased mass effect on the optic chiasm as well as corresponding declines in his vision (light perception only in the left eye; worsening right-sided peripheral vision).
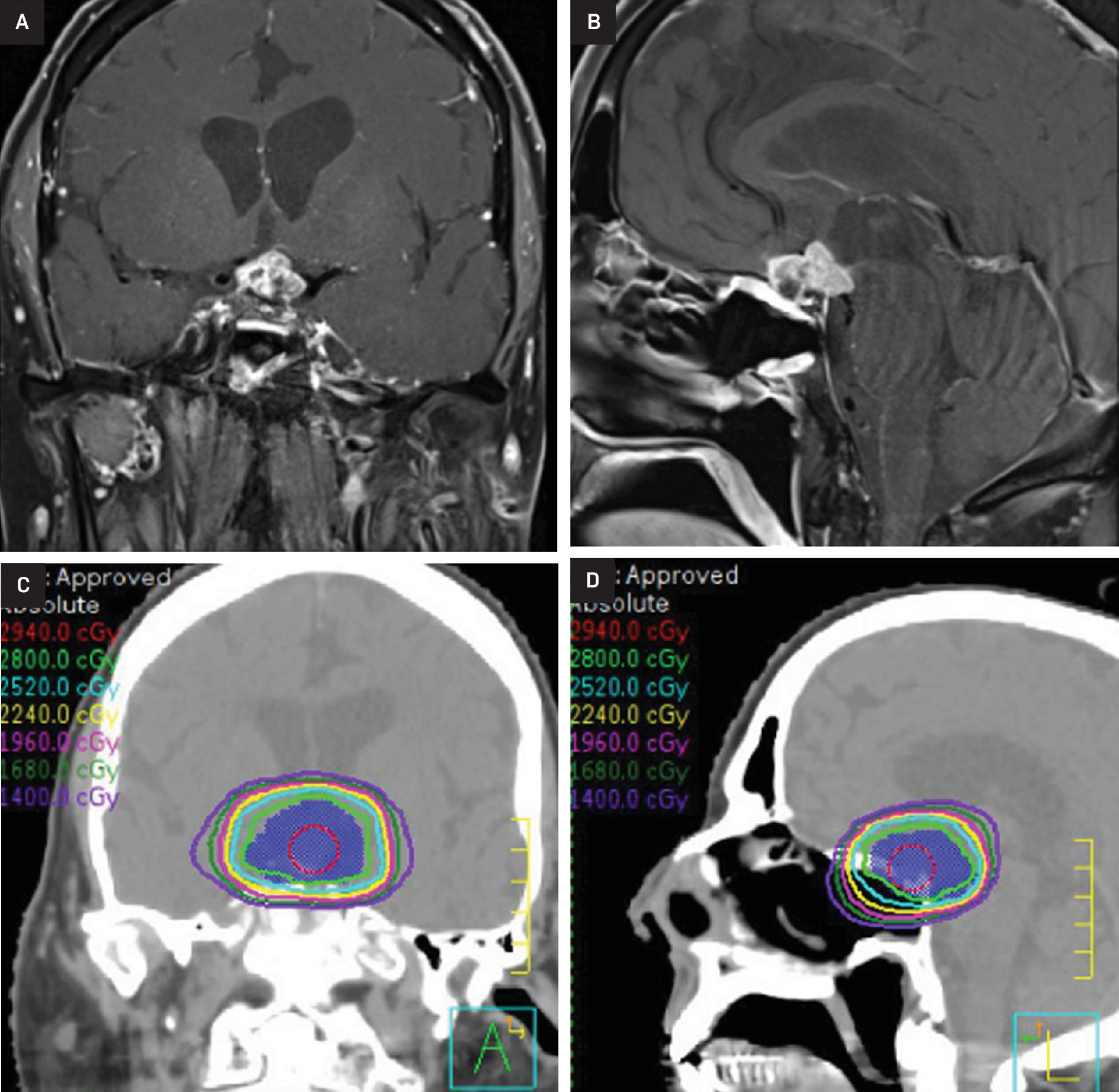
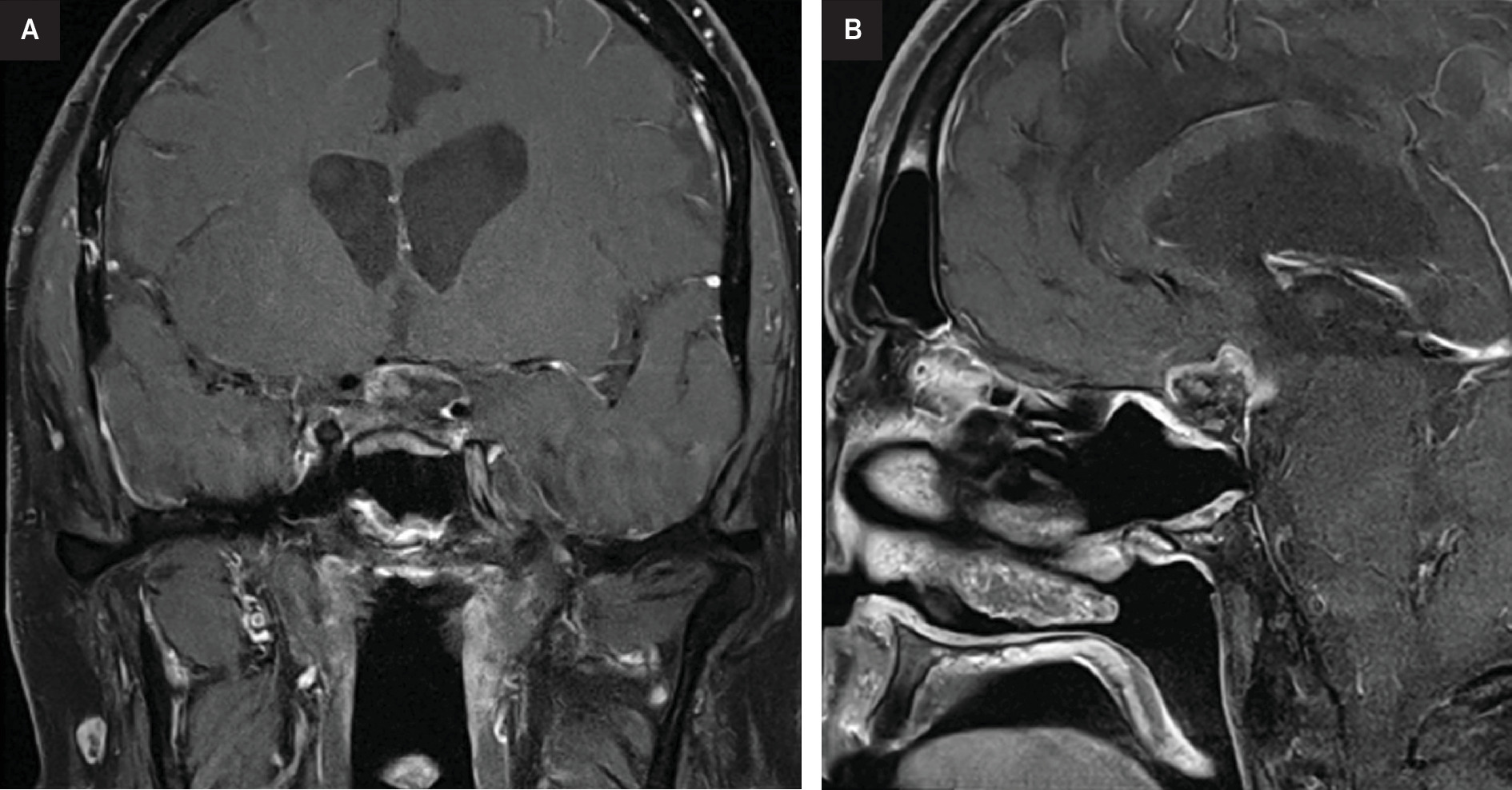
At this time, after a multidisciplinary discussion, the patient was referred to radiation oncology for consideration of additional RT. Ultimately, he was treated to a dose of 28 Gy in 14 fractions using 6 MV photons with 2 non-coplanar VMAT arcs (Figure 2). He again experienced no immediate side effects except for significant fatigue. MRI scans at 3 and 6 months post re-RT demonstrated a decrease in size and enhancement of the suprasellar abnormality with stable vision (Figure 3).
Diagnosis
Lymphocytic hypophysitis.
Differential considerations included neuro-sarcoidosis, pituitary adenoma, central nervous system lymphoma, and craniopharyngioma.
Discussion
Lymphocytic hypophysitis is a rare form of pituitary dysfunction, with some estimates placing its annual incidence at 1 in 9 million.1,2 It is believed to be caused by an autoimmune lymphocytic infiltrate, which leads to destruction of the pituitary gland, often resulting in pan-hypopituitarism.2 While it most commonly occurs in peripartum women, nonpregnant women and men can also be affected.2,3 Individuals with this condition often experience intense headaches and visual changes, with a homogeneously enhancing suprasellar mass appreciated on MRI.3
First-line treatment typically includes high-dose glucocorticoids and/or other systemic therapies such as rituximab, azathioprine, and mycophenolate.1-5 Surgery is usually undertaken for those with disease refractory to medical management. RT utilizing either a conventionally fractionated (1.8-2 Gy per treatment, 12-14 treatments) or stereotactic radiosurgery (12-15 Gy per treatment, 1-2 treatments) approach can be used for medically inoperable patients or for individuals with persistent disease after surgery.3,6-9 Given the rarity of this condition, there is a paucity of data in the literature regarding the use and effectiveness of RT in this setting.3
Recently, Khaleghi et al published on their single-center experience of 3 patients treated with RT for lymphocytic hypophysitis.3 In their systematic review, they were able to identify only 5 other similar cases of lymphocytic hypophysitis treated with radiation. Short-term follow-up limited the analysis of outcomes.
Notably, no patients in the Khaleghi et al series underwent reirradiation with post-RT recurrence.3 To the best of our knowledge, this report represents the first documented case of reirradiation for a patient with multiply recurrent lymphocytic hypophysitis. After an initial course of 24 Gy in 12 fractions, our patient was reirradiated 6 years later to a dose of 28 Gy in 14 fractions. There were no significant side effects associated with the first course of RT, and 2 years post-RT there was radiographic regression and visual improvement. Unfortunately, his response was not sustained, and the patient had symptomatic progression despite medical treatment until re-RT, after which his visual changes and headaches stabilized.
Our patient’s recurrence is somewhat surprising given the general radiosensitivity of lymphocytic cells. Indeed, for this patient, medical management, surgery, and RT have all been ineffective at producing sustained remission of the infiltrate. With reports in the literature suggesting resolution with medical management and/or RT alone, we wonder whether the underlying biology of this patient’s condition is fundamentally different. We have also considered whether stereotactic radiosurgery, and the delivery of ablative doses in just 1 to 2 treatments, would have produced different initial results.6-9 Despite these considerations, we are encouraged by the patient’s initial response to his second course of RT. Our preliminary experience suggests that reirradiation is a safe and effective short-term solution for multiply recurrent lymphocytic hypophysitis. Observation over a more extended period is required to confirm whether these encouraging early results will last over time.
Conclusion
This case report illustrates the short-term feasibility and effectiveness of reirradiation for multiply recurrent lymphocytic hypophysitis. Long-term follow-up is needed to confirm the durability of this approach.
References
- Lin M, Tsang V, Brewer J, Clifton-Bligh R, Gild M. Infiltrative lymphocytic hypophysitis successfully treated with rituximab and mycophenolate mofetil. Endocrinol Diabetes Metab Case Rep. 2020;2020. doi:10.1530/EDM-20-0041.
- Snyder P. Causes of hypopituitarism in UpToDate.
- Khaleghi M, Finger G, Wu K. Successful treatment of medically and surgically refractory lymphocytic hypophysitis with fractionated stereotactic radiotherapy: a single-center experience and systematic literature review. Pituitary. 2024;27(2):213-229. doi:10.1007/s11102-023-01367-8.
- Lecube A, Francisco G, Rodríguez D. Lymphocytic hypophysitis successfully treated with azathioprine: first case report. J Neurol Neurosurg Psychiatry. 2003;74(11):1581-1583. doi:10.1136/jnnp.74.11.1581.
- Schreckinger M, Francis T, Rajah G. Novel strategy to treat a case of recurrent lymphocytic hypophysitis using rituximab. J Neurosurg. 2012;116(6):1318-1323. doi:10.3171/2012.2.JNS111456.
- Leung G, Lopes M, Thorner M, Vance M, Laws E. Primary hypophysitis: a single-center experience in 16 cases. J Neurosurg. 2004;101(2):262-271. doi:10.3171/jns.2004.101.2.0262.
- Pekic S, Bogosavljevic V, Peker S. Lymphocytic hypophysitis successfully treated with stereotactic radiosurgery: case report and review of the literature. J Neurol Surg A Cent Eur Neurosurg. 2018;79(1):77-85. doi:10.1055/s-0037-1604079.
- Ray D, Yen C, Vance M. Gamma knife surgery for lymphocytic hypophysitis. J Neurosurg. 2010;112(1):118-121. doi:10.3171/2009.6.JNS081176.
- Selch M, DeSalles A, Kelly D. Stereotactic radiotherapy for the treatment of lymphocytic hypophysitis. report of two cases. J Neurosurg. 2003;99(3):591-596. doi:10.3171/jns.2003.99.3.0591.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere. The patient has provided informed consent for the publication of this case report.
Citation
. Successful Reirradiation of Multiply Recurrent Lymphocytic Hypophysitis: A Case Report. Applied Radiation Oncology. 2026. doi:10.37549/ARO-D-26-0002.