Stereotactic Radiosurgery and Immunotherapy for Melanoma and NSCLC Brain Metastases: Practical Integration, Timing, and Toxicity
Applied Radiation Oncology — Vol. 15, Issue 2
Published: June 1, 2026
1 British Columbia Cancer Agency, Abbotsford, British Columbia, Canada
* Corresponding author: Rahul Barve (drrahulbarve@gmail.com)
Abstract
Keywords
stereotactic radiosurgery, immunotherapy, brain metastases, immune checkpoint inhibitors, melanoma, non-small cell lung cancer, radionecrosis, treatment timing, V12 Gy, hypofractionation
Introduction
Brain metastases occur in up to 20%-40% of patients with advanced solid malignancies and remain a major cause of neurologic morbidity and mortality.1 The incidence is particularly high in melanoma, non-small cell lung cancer (NSCLC), and renal cell carcinoma (RCC), reflecting tumor biology and improved systemic therapies that prolong survival.2 Although breast cancer is also a common source, it is not emphasized here due to the evolving role of immune checkpoint inhibitors (ICIs) in this setting.3,4 Over the past decade, management has shifted toward focal therapies such as stereotactic radiosurgery (SRS) rather than whole-brain radiation therapy (WBRT) in appropriately selected patients.5
SRS is a standard treatment for brain metastases, delivering highly conformal ablative doses with excellent local control while preserving neurocognitive function.6 Recent randomized data suggest that, in selected patients with multiple brain metastases, SRS may provide superior cognitive outcomes compared with hippocampal avoidance WBRT.7 Concurrently, ICIs have transformed systemic therapy for melanoma, NSCLC, and other malignancies with central nervous system involvement.8 As a result, patients increasingly receive both SRS and ICIs during their treatment course.9
This convergence raises a key clinical question: how should SRS and ICIs be optimally integrated, and does treatment timing influence outcomes and toxicity? The rationale for combination is biologically compelling. Radiation enhances tumor immunogenicity through antigen release, dendritic cell activation, and T-cell priming, potentially synergizing with checkpoint blockade.10 However, this immune activation may also increase inflammatory toxicity, including radiation necrosis (RN) and edema.11
Despite expanding clinical experience, optimal sequencing remains uncertain. Current evidence is largely retrospective and heterogeneous, with variable definitions of “concurrent” therapy and differences in histology and treatment regimens. Nonetheless, consistent patterns suggest improved intracranial outcomes with concurrent treatment and highlight important toxicity differences between single-agent and dual ICI strategies.12,13
This narrative review provides a clinically focused synthesis of the evidence on SRS-ICI integration in brain metastases, emphasizing biologic rationale, treatment timing, efficacy, and toxicity. We also propose a practical framework for clinical decision-making and highlight key areas for future research.
Methods of Literature Review
This narrative review was conducted using focused searches of PubMed, Embase, and Scopus. Search terms included combinations of “brain metastases,” “stereotactic radiosurgery,” “stereotactic radiation therapy,” “immune checkpoint inhibitors,” “PD-1,” “PD-L1,” “CTLA-4,” “timing,” “concurrent,” “sequential,” and “radionecrosis.”
Priority was given to multicenter studies, contemporary retrospective analyses, prospective trials, and meta-analyses published between 2016 and 2026. Studies evaluating treatment timing, local control, overall survival, and RN were included, with emphasis on melanoma and NSCLC cohorts.
Biological Rationale for Combining SRS and Immunotherapy
The rationale for combining SRS with ICIs is based on radiation-induced immune modulation.10 High-dose focal radiation promotes immunogenic cell death, enhancing antigen release, dendritic cell activation, and T-cell priming, thereby transforming the irradiated lesion into an in situ vaccine-like stimulus.14,15
Radiation also modulates the tumor microenvironment by increasing major histocompatibility complex expression, enhancing T-cell infiltration, and altering cytokine signaling.16 These effects may augment ICI efficacy, which functions by relieving inhibitory signals on T cells and sustaining antitumor immune responses.17 This biologic synergy supports combining SRS and ICIs, particularly when delivered in close temporal proximity.18-20
However, these same mechanisms may also increase toxicity. RN is a multifactorial process involving vascular injury, hypoxia, and immune-mediated inflammation.21 ICIs may amplify these pathways, particularly with dual checkpoint blockade, potentially increasing the risk of treatment-related toxicity.11
Clinical Evidence on Treatment Timing
Definition of Concurrent Treatment
A major limitation in the literature is the lack of a standardized definition of “concurrent” treatment. Definitions vary across studies, ranging from within 1, 2, or 4 weeks to within one pharmacokinetic half-life of the ICI agent.19
Despite this variability, most studies adopt a practical definition of concurrent therapy as SRS delivered within approximately 2 to 4 weeks of ICI administration.9,13 Some analyses suggest that shorter intervals, particularly within 2 weeks or one half-life, may be associated with improved intracranial response, although optimal timing remains uncertain.19
Evidence in Melanoma
The emergence of dual checkpoint blockade has significantly altered the management of melanoma brain metastases.22 Prospective phase II studies have demonstrated durable intracranial activity with nivolumab plus ipilimumab in asymptomatic patients. In CheckMate 204, Tawbi et al reported an intracranial objective response rate of 57%, establishing dual checkpoint blockade as a highly active systemic therapy for untreated melanoma brain metastases.23 Long-term follow-up demonstrated durable benefit, with 3-year intracranial progression-free survival and overall survival rates of 54.1% and 71.9%, respectively.24 Similarly, the randomized phase II ABC trial showed superior intracranial response and long-term survival with nivolumab plus ipilimumab compared with nivolumab alone, supporting dual checkpoint blockade as the preferred systemic approach in asymptomatic patients.25 These findings have raised important questions regarding the optimal integration of SRS, which are being addressed in the ongoing ABC-X trial evaluating nivolumab plus ipilimumab with or without concurrent intracranial SRS.26
Against this backdrop of highly effective systemic therapy, multiple retrospective studies have evaluated whether the addition and timing of SRS further improve intracranial outcomes. Kotecha et al reported that timing influences efficacy more than toxicity, with concurrent ICI improving response and low RN (3%-5%),19 while Carron et al confirmed low toxicity with anti-PD-1 therapy (adverse radiation effect 4%-5%, symptomatic <3%).27
Regimens incorporating CTLA-4 inhibition, particularly dual ICI, are associated with higher RN rates, although estimates vary. Minniti et al reported moderate RN (15%-25%) with concurrent nivolumab/ipilimumab.28 In contrast, Tang et al demonstrated significantly improved local control (92% vs 64%) without excess toxicity or increased RN.29 Fu et al similarly observed improved survival with concurrent SRS-ICI (37.1 vs 11.4 months) without increased radiation toxicity (2%-3%).30 More recent data from Messing et al show excellent local control (90%) with low symptomatic RN (7%), while identifying prior systemic therapy as a prognostic factor.31 Conversely, Vaios et al reported higher RN rates with dual ICI (20%-25%),11 whereas Mandalà et al demonstrated survival benefit with moderate RN (10%).32 Key retrospective studies are summarized in Table 1.
| Study | Sample Size | ICI Regimen | Treatment Arms | Timing Definition | RN Definition | RN Risk | Key Efficacy + Survival Outcome | Key Takeaway |
|---|---|---|---|---|---|---|---|---|
| Kotecha et al19 | 150 pts /1003 lesions | PD-1 dominant | SRS + ICI (timing cohorts) | Immediate vs concurrent vs delayed | Radiographic RN; symptomatic cases reported separately | 3.2%-3.5%; 7 symptomatic cases | CR ↑ (50% vs 32%); durable response ↑ (94% vs 71%); OS ~30 mo | Timing > toxicity; immediate/concurrent optimal; steroids detrimental |
| Minniti et al28 | 80 pts / 326 lesions | PD-1 vs CTLA-4 | SRS + nivolumab; SRS + ipilimumab | Concurrent (~1 wk) | MRI/F-DOPA PET-defined RN; Grade 3 RN separately reported | 20% (Nivo) vs 29% (Ipi); Grade 3 RN: 9% vs 11% | PFS/LC/OS favor PD-1; OS 22 vs 14.7 mo | PD-1-based SRS associated with better outcomes; higher RN with CTLA-4 |
| Carron et al27 | 50 pts / 188 lesions | PD-1 only | SRS + anti-PD-1 | Concurrent ≤3 mo | MRI defined ARE; symptomatic subset reported | 4.4% of lesions (8/181); 14.6% of patients (7/48); 6 symptomatic cases (12.5%) | PFS ~13 mo; OS ~16.6 mo (1-yr ~60%) | Favorable survival with low RN; safe PD-1 + SRS |
| Tang et al29 | 49 pts / 158 lesions | Dual ICI | Nivo + Ipi ± SRS | Concurrent (median 8 d; within 6 wk) | Symptomatic RN only; pathologic confirmation or multidisciplinary review; | 6.0% (5/84 lesions) | LC ↑ (92% vs 64%); OS similar (~72% vs 71% at 1 yr) | SRS improves LC without added toxicity; no OS benefit |
| Fu et al30 | 98 pts | ICI | Concurrent vs non-concurrent SRS + ICI | ≤4 wk | CTCAE CNS necrosis/ARE; symptomatic status not specified | 2% (concurrent) vs 3% (non-concurrent) | OS ↑ (37 vs 11 mo); PFS ↔ | Concurrent ICI improves OS without ↑ RN; edema slightly ↑ |
| Vaios et al11 | 288 pts / 1704 lesions | Dual vs single/no ICI | SRS + dual vs single vs none | Concurrent ≤4 wk | CTCAE grade ≥2 symptomatic RN only; pathologic or clinical-radiographic diagnosis | 21.8% (dual ICI) vs 13.5% (single ICI); no ICI 13.7% | RN associated with worse OS | Dual ICI significantly increases RN risk |
| Mandalà et al32 | 453 pts | Dual ICI (Nivo + Ipi) | Dual ICI ± SRT | Concomitant ≤2 wk | MRI defined RN with clinical follow-up; symptomatic status not specified | 10.3% (10.9% sequential vs 9.3% concomitant) | OS ↑ with SRT (27.3/22.2 vs 9.4 mo); no difference between concomitant vs sequential SRT | SRT improves OS regardless of timing |
| Messing et al31 | 68 pts / 413 lesions | Dual ICI (Nivo + Ipi) | SRS + concurrent dual ICI | ≤8 wk | MRI perfusion/permeability sequences, MR spectroscopy, symptomatic RN only | 7% (5 patients) | OS 24 mo; 12-mo 64%, 24-mo 50%; LC ~ 89% | Durable control; prior ICI/targeted therapy predicts worse outcomes |
Overall, evidence is heterogeneous and predominantly retrospective yet supports close temporal integration of SRS and ICI to optimize intracranial control. ICI regimen and prior therapy exposure may influence toxicity and outcomes, warranting prospective validation.
Evidence in NSCLC
NSCLC has a growing but less mature evidence base for SRS-ICI integration compared with melanoma. Early-phase prospective studies demonstrate feasibility, safety, and encouraging intracranial control.33-36
Across retrospective cohorts, SRS combined with ICI has consistently been associated with improved intracranial control and, in some studies, overall survival. Foundational studies by Chen et al and Schapira et al demonstrated superior survival and intracranial control with concurrent SRS-ICI (within 2-4 wk) compared with nonconcurrent approaches.13,37 Larger analyses, including Yomo et al, confirmed improved survival (mOS 16.9 vs 12.0 mo) and intracranial PFS without increased toxicity, findings that were also supported by Bashir et al.38,39
Some studies have highlighted differential response patterns. Shepard et al reported higher complete response rates with concurrent ICI (50% vs 15.6%) without a survival benefit,40 while Singh et al demonstrated greater tumor shrinkage in larger lesions (>500 mm³), suggesting size-dependent synergy.41 Concurrent therapy has also been associated with improved distant intracranial control, particularly with shorter treatment intervals (≤7 d).42,43 More recent studies by Dohm et al, Frehner et al, and Lu et al further support improved intracranial response with upfront or concurrent SRS, although overall survival benefits remain inconsistent, suggesting a potential role for selective or deferred radiation in asymptomatic patients.44-46 Key retrospective studies are summarized in Table 2.
| Study | Sample Size | ICI Regimen | Treatment Arms | Timing Definition | RN Definition | RN Risk | Key Efficacy + Survival Outcome | Key Takeaway |
|---|---|---|---|---|---|---|---|---|
| Yomo et al38 | 585 pts | Mixed ICIs | SRS + ICI vs SRS | Concurrent ≤3 mo | CTCAE v4.0 toxicity grading used | One grade 4 RN, 5 grade 3 RN | mOS 16.9 vs 12.0 mo; HR 0.62; IC-PFS ↑ (35% vs 26%) | Concurrent SRS-ICI associated with improved OS and IC-PFS without ↑ toxicity |
| Shepard et al40 | 51 pts | PD-1/PD-L1 | SRS + ICI vs SRS | ICI within 3 mo | Radiographic RN; included symptomatic RN | Symptomatic RN 2.9% (1/34); no increased RN or intratumoral hemorrhage risk with concurrent ICI | No OS/PFS benefit; CR ↑ (50% vs 15.6%); faster regression | Improved radiographic response without survival benefit |
| Singh et al41 | 85 pts | Anti–PD-1 | SRS + ICI vs SRS + chemo | Variable (subset ≤4 wk) | RN confirmed by histopathology or imaging changes | RN: 10.2% (4/39) vs 10.9% (5/46) (P = 0.7) | No OS benefit (10 vs 11.6 mo); large lesions ( >500 mm³) response ↑ (90% vs 47.8%) | Benefit limited to larger lesions; no overall survival advantage |
| Singh et al42 | 99 pts | PD-1/PD-L1 | SRS + ICI vs SRS + chemo vs SRS + TKI | Concurrent ≤30 d | RN defined by pathology or multidisciplinary MRI review | RN in 34/136 SRS sessions (25%); no increased RN risk with ICI. | 1-yr DI-PFS ↑ (67% vs 37% vs 39%); PD-L1 ≥50%: 80% | Concurrent ICI improves intracranial control, especially PD-L1-high |
| Frehner et al45 | 128 pts | ICI ± chemo | ICI ± chemo + upfront SRT vs ICI ± chemo | Upfront SRT vs none | CTCAE v5.0 CNS adverse events recorded; included symptomatic RN | Symptomatic RN 3.4% (2/58); no fatal CNS adverse events. | iPFS ↑ (12.6 vs 8.2 mo; HR 0.62); no OS benefit (22.8 vs 21.7 mo) | Upfront SRT improves intracranial control; deferral feasible without OS compromise |
| Chung et al47 | 82 pts | ICI/TKI | Reduced-dose vs standard-dose SRS | Concurrent ≤30 d | Radiographic AREs (radiation necrosis + edema) assessed | AREs: 10.8% vs 23.7% (P = 0.020) | LC similar (94.6% vs 90.3%) | Dose reduction maintains control with lower toxicity |
Importantly, RN and adverse radiation effects remain low (3%-10%) and are not consistently increased with ICI. Established dosimetric factors, particularly V12 Gy, appear to remain the primary drivers of radionecrosis (RN) risk in patients receiving ICIs.47
Evidence in RCC
RCC represents a distinct clinical scenario compared with melanoma and NSCLC. Although ICI have improved outcomes in metastatic RCC, intracranial activity remains modest, and local therapy continues to play a central role.48,49 In the NIVOREN study, nivolumab monotherapy demonstrated limited intracranial efficacy, with an intracranial response rate of 12% and median intracranial progression-free survival of 2.7 months.48 In contrast, CheckMate 920 reported improved outcomes with nivolumab plus ipilimumab, achieving an objective response rate of 32% and median progression-free survival of 9.0 months in patients with asymptomatic brain metastases.49 Consequently, SRS remains a cornerstone of management for RCC brain metastases.50,51 Emerging retrospective data suggest that concurrent SRS and ICI may improve intracranial control and survival without substantially increasing RN risk.9,13,52 Concurrent ICI has not been associated with increased symptomatic RN, and dosimetric factors such as V12 Gy appear to remain the primary determinants of toxicity.9,53 However, prospective data defining the optimal integration of SRS and immunotherapy in RCC remain limited.
Evidence From Pooled and Meta-Analyses
Pooled and meta-analytic evidence supports combining SRS with ICI, with stronger and more consistent benefit in melanoma than NSCLC. In melanoma, systematic reviews highlight a shift toward multimodal, patient-specific strategies integrating SRS, immunotherapy, and systemic therapy.54 In melanoma, meta-analyses demonstrate significant survival benefit with SRS-ICI, particularly with anti-PD-1 regimens,55 while Bayesian network analyses rank SRS + ICI as the most effective strategy for overall survival and intracranial control, albeit with increased RN risk.56 Timing analyses further suggest that concurrent SRS-ICI (within 4 wk) improves survival and intracranial outcomes compared with nonconcurrent approaches.12,57
Contemporary pooled data report high local control (80%-85%) and favorable 1-year survival (65%-70%), with RN rates of approximately 10% to 12% in the modern immunotherapy era.58 Importantly, large multicenter analyses indicate that RN risk is primarily driven by dosimetric factors, particularly V12 Gy, rather than treatment timing, supporting the safety of concurrent approaches when appropriate constraints are applied.9
In NSCLC, pooled data suggest a more nuanced interaction. Chu et al found no survival advantage with the addition of cranial radiation therapy to ICI, although concurrent treatment reduced distant brain failure.59 In contrast, Yang et al demonstrated improved overall survival with combined radiation therapy and ICI compared with radiation therapy alone, with concurrent treatment emerging as the optimal strategy without increased toxicity.60 Collectively in NSCLC, these findings suggest that immunotherapy is the primary driver of survival, whereas SRS primarily enhances intracranial disease control. Major pooled analyses are summarized in Table 3.
| Study | Predominant Histology | Sample Size | ICI Regimen | Treatment Arms | Risk of Radionecrosis | Efficacy and Survival Outcome | Key Takeaways |
|---|---|---|---|---|---|---|---|
| Lehrer et al12 | Mixed (melanoma dominant) | 17 studies; 534 pts | CTLA-4, PD-1 | Concurrent vs non-concurrent SRS + ICI | RN ~5.3% | 1-yr OS: 64.6% vs 51.6%; improved LC | Early evidence supporting concurrent SRS + ICI |
| Badrigilan et al57 | Predominantly melanoma | 16 studies; 1356 pts | Mostly CTLA-4, some PD-1 | SRS + ICI vs SRS; timing comparisons | No significant increase | Improved OS and local control | Supports concurrent strategy without clear toxicity increase |
| Chu et al59 | NSCLC | 46 trials; 3160 pts | PD-1, PD-L1, CTLA-4 | ICI vs ICI + RT; SRS vs WBRT | Not primary endpoint | PFS HR ~0.48; OS HR ~0.64; ↓ DBF (OR 0.15) | ICI drives survival; RT improves intracranial control |
| Yang et al60 | NSCLC | 19 studies | PD-1/PD-L1/CTLA-4 | RT + ICI vs RT alone | No ↑ grade 3-4 toxicity | OS improved (HR ~0.77 vs RT alone) | Adding ICI to RT improves survival |
| Lehrer et al12 | Mixed (melanoma, NSCLC, RCC) | 657 pts; 4182 mets | PD-1, PD-L1, CTLA-4 | Concurrent vs non-concurrent SRS + ICI | RN ~ 10 %; symptomatic ~6%-7% | No major OS difference by timing | RN driven by dosimetry (V12 Gy) |
| Williams et al55 | Melanoma | 126 studies; ~6500 pts | Anti–PD-1, CTLA-4, mixed | SRS + ICI vs SRS or ICI alone | Not consistently reported | ~30%-65% reduction in mortality risk | Strong survival benefit with SRS + ICI |
| Li et al56 | Melanoma | 10 studies; 836 pts | ICI ± targeted therapy | SRS + ICI vs SRS alone or ICI alone | Higher RN risk with SRS + ICI vs SRS alone | OS improved vs SRS alone (HR ~0.64); intracranial PFS improved vs ICI alone (HR ~0.66) | SRS + ICI ranked best for OS and intracranial control |
| Grant et al54 | Melanoma | 70 studies | ICI, targeted therapy | Multimodal approaches | Low neurotoxicity | mOS ~5-16 months | Supports multimodal integration |
| Ahmadvand et al58 | Mixed | 16 studies; 1529 pts | PD-1/PD-L1 inhibitors | SRS + ICI | RN ~12 %; ARE ~31% | LC ~84% (12 mo); 1-yr OS ~67% | High control with measurable RN risk |
Comparative Considerations: Melanoma vs NSCLC
Important distinctions exist between melanoma and NSCLC in the context of SRS-ICI integration. In melanoma, evidence consistently supports a synergistic benefit, particularly with concurrent treatment.12,55,56 In NSCLC, outcomes are more heterogeneous, with immunotherapy driving survival and radiation therapy contributing primarily to intracranial control in a context-dependent manner.59,60 Molecular subgroups further influence treatment decisions; tumors with actionable driver mutations (e.g., EGFR, ALK) often respond well to CNS-penetrant targeted therapies,61 and these mutations are less responsive to ICI,62 limiting the role in SRS-ICI integration in this entity. In these cases, SRS is typically reserved for oligoprogressive or symptomatic disease.
Role of Dosimetry and Treatment Factors
RN following SRS is multifactorial and cannot be attributed to treatment timing alone. While much of the literature focuses on the temporal relationship between SRS and ICI, radiation dose-volume parameters appear to remain the primary determinants of toxicity, particularly with combined-modality therapy.
Among dosimetric parameters, the volume of normal brain receiving 12 Gy (V12 Gy) is the most robust and consistently validated predictor of RN. In a large multicenter analysis by Lehrer et al including 657 patients and over 4000 brain metastases, V12 Gy was independently associated with RN risk, not the timing of ICI administration.9 Increasing V12 Gy correlates with stepwise toxicity, with low-risk (<12 cm³), intermediate-risk (12-20 cm³), and high-risk (>20 cm³) groups demonstrating progressively higher rates.9 These findings underscore that dosimetric optimization remains the primary determinant of RN risk, even in the era of immunotherapy.
Additional dosimetric and treatment-related factors contribute to the risk of RN. Treatment of larger lesions (typically >2 cm) requires higher integral dose and results in greater exposure of surrounding normal brain tissue.47,63,64 In patients with multiple brain metastases, cumulative treated volume increases overall brain dose and expands the low-dose radiation bath.65 Prior cranial irradiation, including previous SRS or WBRT, further reduces normal tissue tolerance and may further increase the risk of RN.66
Clinical factors, including baseline edema, corticosteroid use, and lesion location, particularly in eloquent or deep brain regions, may influence both the risk and clinical impact of RN.67,68 These factors may interact with immunotherapy, as immune activation can amplify inflammatory responses.
Overall, these findings support a shift in clinical thinking. RN risk should not be viewed solely through treatment timing, but rather through an integrated framework incorporating dosimetry, lesion characteristics, prior treatment, and immunotherapy regimen. In particular, patients with high-risk dosimetric features (e.g., elevated V12 Gy or large target volume) combined with clinical modifiers such as dual checkpoint blockade or significant perilesional edema may warrant treatment modification strategies, including dose optimization and hypofractionation.
Fractionation and Risk Mitigation Strategies
Hypofractionated stereotactic radiation therapy is commonly employed to mitigate the risk of RN, particularly for lesions >2 cm or when V12 Gy exceeds approximately 10 cm³,64 or those receiving dual immune checkpoint inhibition.9 Although prospective data remain limited, this approach is widely adopted in clinical practice. By reducing peak dose to normal brain tissue, fractionation may help offset the increased inflammatory effects associated with concurrent immunotherapy.
Radiographic Assessment and Diagnostic Challenges
Distinguishing pseudoprogression, RN, and true tumor progression after SRS in patients receiving ICIs remains a major diagnostic challenge, as all may present with enlarging contrast-enhancing lesions on MRI.69,70 Pseudoprogression typically occurs early in the first few months (approximately 6 months), whereas RN is a delayed effect, often developing 6 to 12 months post SRS.71-73 The combined inflammatory effects of SRS and immunotherapy further complicate interpretation. The iRANO criteria recommend confirmatory imaging within 6 months of ICI initiation.74 Advanced imaging modalities, including perfusion MRI and amino acid PET, improve diagnostic accuracy, though uncertainty often necessitates multidisciplinary evaluation and serial imaging.69 Amino acid PET tracers, particularly fluoroethyltyrosine PET and methionine PET, provide greater specificity than conventional MRI for distinguishing RN from tumor progression and are increasingly used in contemporary diagnostic algorithms.69,75,76
Comparison of reported RN rates across studies is limited by heterogeneity in diagnostic criteria and outcome definitions. Some studies report only symptomatic RN, whereas others include asymptomatic radiographic changes or broader adverse radiation effects, likely contributing to variability in reported RN incidence. Studies reporting only symptomatic RN generally demonstrate lower rates than those incorporating radiographic or asymptomatic RN. Therefore, RN rates should be interpreted with caution when comparing outcomes across studies.
Management of RN
Management of RN after SRS follows a stepwise, symptom-guided approach. Asymptomatic cases may be observed with serial imaging, while symptomatic patients are treated with corticosteroids using the lowest effective dose and gradual taper. Bevacizumab is effective in steroid-refractory cases, with response rates exceeding 80% and significant radiographic improvement.77-79 Emerging evidence suggests that Boswellia serrata reduces RN-associated edema, with a retrospective series reporting radiographic improvement in approximately 60% of patients and a favorable safety profile, although prospective validation is needed.80 Surgical resection or laser interstitial thermal therapy (LITT) is reserved for refractory or diagnostically uncertain cases, providing tissue confirmation and durable control.81 Emerging data suggest comparable efficacy between bevacizumab and LITT.82 Management should be individualized based on symptoms, lesion characteristics, and diagnostic certainty.
Limitations of Current Evidence
The current literature is limited by its predominantly retrospective nature, heterogeneity in study design, and variability in definitions of concurrent treatment. Confounding by indication and challenges in distinguishing RN from tumor progression further complicate interpretation.
Practical Clinical Implications
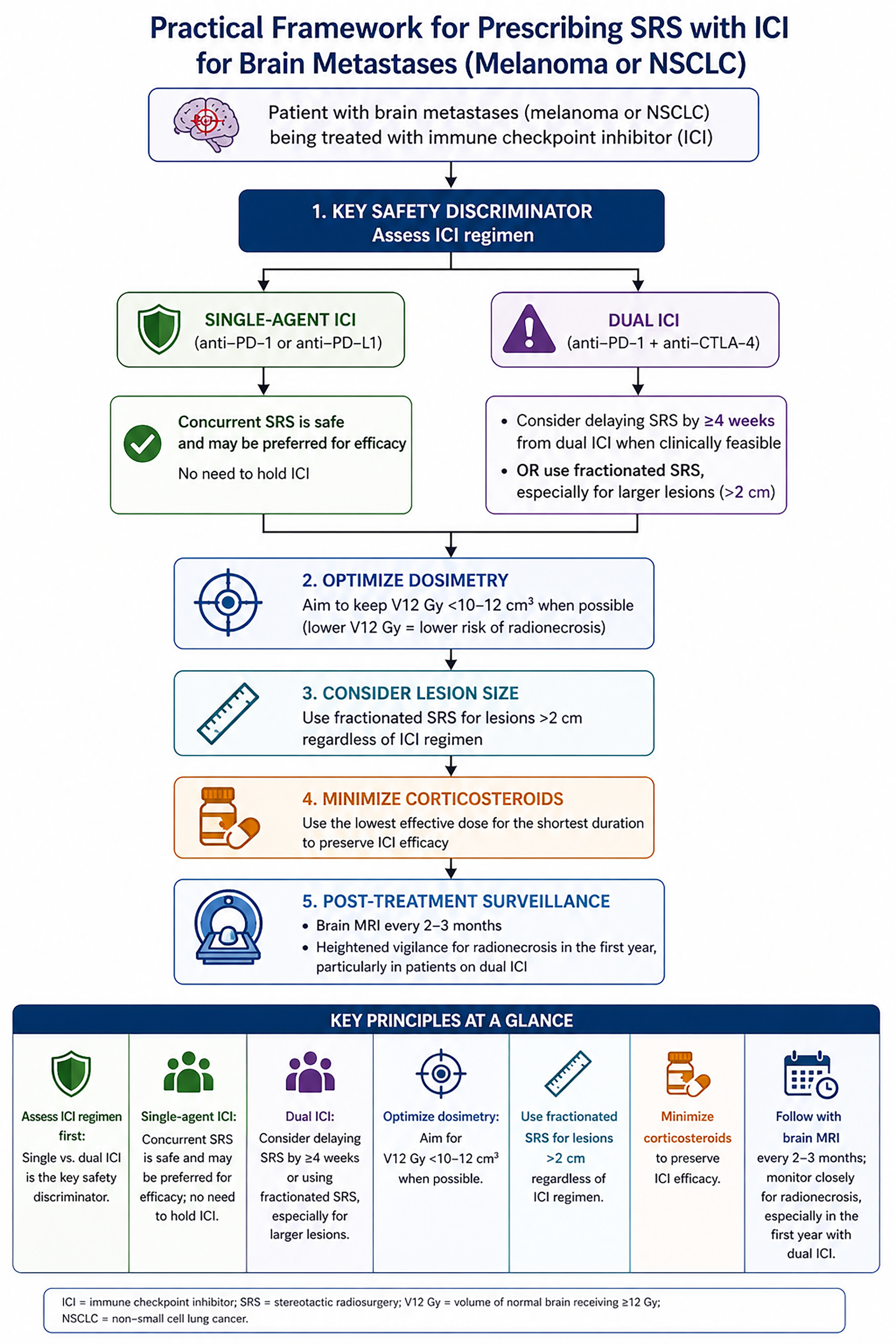
The integration of SRS with ICI in clinical practice requires a structured, risk-adapted approach that incorporates immunotherapy regimen, dosimetric parameters, lesion characteristics, and patient-specific factors.
Concurrent SRS with single-agent ICI is generally well tolerated and may enhance local control without a substantial increase in RN risk.19 In this context, concurrent or near concurrent SRS, typically within 2 to 4 weeks, is a reasonable and commonly adopted approach. In contrast, dual checkpoint blockade may be associated with an increased risk of symptomatic RN in some studies, although the evidence remains heterogeneous and warrants a more cautious integration strategy.11 For these patients, delayed SRS by ≥4 weeks or the use of hypofractionated regimens should be considered, particularly for larger lesions or those with high-risk features.11
The volume of normal brain receiving 12 Gy (V12 Gy) has been one of the most consistently validated predictors of RN in SRS literature and remains highly relevant in patients receiving concurrent immunotherapy.9 Efforts to minimize normal brain dose are essential, with V12 Gy thresholds serving as a practical guide for risk stratification. Hypofractionated SRS should be considered for lesions greater than 2 cm83 or when V12 Gy constraints cannot be met, particularly in patients receiving dual ICI.
Additional factors, including baseline edema, corticosteroid use, prior cranial irradiation, and intracranial disease burden, may influence efficacy and toxicity and should inform individualized treatment planning. Minimizing corticosteroid exposure is particularly important given its potential impact on immunotherapy efficacy.84
Overall, optimal integration of SRS and ICI requires a composite clinical framework that prioritizes immunotherapy regimen, dosimetric risk, and lesion characteristics rather than relying on treatment timing alone. A practical decision-making framework is summarized in (Figure 1).
Future Directions
Future research efforts should focus on prospective trials to define optimal timing and sequencing, alongside strategies such as dose de-escalation and fractionation to reduce toxicity.25,47 Emerging biomarkers, including neutrophil-to-lymphocyte ratio, early CD8+ T-cell activation, tumor aneuploidy, and immune-inflammatory signatures, may help identify patients most likely to benefit from combined therapy and guide immunotherapy selection.16,85 Additional areas include exploiting the abscopal effect,86 novel immune targets, advanced imaging, and multimodality approaches.87-89
Conclusion
The integration of SRS and ICIs represents a major advance in the management of brain metastases. Concurrent SRS with single-agent ICI appears feasible and may enhance intracranial control without significantly increasing toxicity. In contrast, dual checkpoint blockade and higher dose volume exposure (particularly V12 Gy) define a higher-risk population for RN, necessitating more cautious, individualized strategies. Optimal integration requires consideration of not only timing, but also immunotherapy regimen, lesion characteristics, fractionation, and dosimetric parameters. Prospective studies are needed to define these relationships and guide evidence-based clinical decision-making.
References
- Lamba N, Wen P, Aizer A. Epidemiology of brain metastases and leptomeningeal disease. Neuro Oncol. 2021;23(9):1447-1456. doi:10.1093/neuonc/noab101.
- Cagney D, Martin A, Catalano P. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study. Neuro Oncol. 2017;19(11):1511-1521. doi:10.1093/neuonc/nox077.
- Zou Y, Wu J, Yuan Z, He X, Tang H. Targeting the neuro-immune crosstalk in breast cancer brain metastases. J Immunother Cancer. 2026;14(4). doi:10.1136/jitc-2025-014134.
- Schlam I, Gatti-Mays M. Immune checkpoint inhibitors in the treatment of breast cancer brain metastases. Oncologist. 2022;27(7):538-547. doi:10.1093/oncolo/oyac064.
- Vogelbaum M, Brown P, Messersmith H. Treatment for brain metastases: ASCO-SNO-ASTRO guideline. J Clin Oncol. 2022;40(5):492-516. doi:10.1200/JCO.21.02314.
- Cherng H, Sun K, Bentzen S. Redefining neurocognitive outcomes after radiation for brain metastases: a patient-level meta-analysis of recovery following initial decline. J Natl Cancer Inst. 2026;118(2):269-275. doi:10.1093/jnci/djaf264.
- Aizer A, Shin K, Catalano P. Treatment for brain metastases with stereotactic radiation vs hippocampal-avoidance whole brain radiation: a randomized clinical trial. JAMA. 2026;335(13):1127-1136. doi:10.1001/jama.2026.0076.
- Aquilanti E, Brastianos P. Immune checkpoint inhibitors for brain metastases: a primer for neurosurgeons. Neurosurgery. 2020;87(3). doi:10.1093/neuros/nyaa095.
- Lehrer E, Kowalchuk R, Gurewitz J. Concurrent administration of immune checkpoint inhibitors and single fraction stereotactic radiosurgery in patients with non-small cell lung cancer, melanoma, and renal cell carcinoma brain metastases. Int J Radiat Oncol Biol Phys. 2023;116(4):858-868. doi:10.1016/j.ijrobp.2023.01.017.
- Yoo K, Park D, Choi J. Optimizing the synergy between stereotactic radiosurgery and immunotherapy for brain metastases. Front Oncol. 2023;13. doi:10.3389/fonc.2023.1223599.
- Vaios E, Shenker R, Hendrickson P. Symptomatic necrosis with dual immune-checkpoint inhibition and radiosurgery for brain metastases. JAMA Netw Open. 2025;8(4). doi:10.1001/jamanetworkopen.2025.4347.
- Lehrer E, Peterson J, Brown P. Treatment of brain metastases with stereotactic radiosurgery and immune checkpoint inhibitors: an international meta-analysis of individual patient data. Radiother Oncol. 2019;130:104-112. doi:10.1016/j.radonc.2018.08.025.
- Chen L, Douglass J, Kleinberg L. Concurrent immune checkpoint inhibitors and stereotactic radiosurgery for brain metastases in non-small cell lung cancer, melanoma, and renal cell carcinoma. Int J Radiat Oncol Biol Phys. 2018;100(4):916-925. doi:10.1016/j.ijrobp.2017.11.041.
- Portella L, Scala S. Ionizing radiation effects on the tumor microenvironment. Semin Oncol. 2019;46(3):254-260. doi:10.1053/j.seminoncol.2019.07.003.
- Jansen C, Pagadala M, Cardenas M. Pre-operative stereotactic radiosurgery and peri-operative dexamethasone for resectable brain metastases: a two-arm pilot study evaluating clinical outcomes and immunological correlates. Nat Commun. 2024;15(1):8854. doi:10.1038/s41467-024-53034-6.
- Lynch C, Pitroda S, Weichselbaum R. Radiotherapy, immunity, and immune checkpoint inhibitors. Lancet Oncol. 2024;25(8). doi:10.1016/S1470-2045(24)00075-5.
- Fukumura K, Jiang P, Yeboa D. Ionizing radiation enhances prognostically significant cellular immunity programs in the brain metastasis microenvironment. Clinical Cancer Research. 2026;32(11):2305-2316. doi:10.1158/1078-0432.CCR-25-3525.
- Sharabi A, Lim M, DeWeese T, Drake C. Radiation and checkpoint blockade immunotherapy: radiosensitisation and potential mechanisms of synergy. Lancet Oncol. 2015;16(13). doi:10.1016/S1470-2045(15)00007-8.
- Kotecha R, Kim J, Miller J. The impact of sequencing PD-1/PD-L1 inhibitors and stereotactic radiosurgery for patients with brain metastasis. Neuro Oncol. 2019;21(8):1060-1068. doi:10.1093/neuonc/noz046.
- Qian J, Martin A, Martin K. Response rate and local recurrence after concurrent immune checkpoint therapy and radiotherapy for non-small cell lung cancer and melanoma brain metastases. Cancer. 2020;126(24):5274-5282. doi:10.1002/cncr.33196.
- Vaios E, Winter S, Shih H. Novel mechanisms and future opportunities for the management of radiation necrosis in patients treated for brain metastases in the era of immunotherapy. Cancers. 2023;15(9). doi:10.3390/cancers15092432.
- Kalaora S, Nagler A, Wargo J, Samuels Y. Mechanisms of immune activation and regulation: lessons from melanoma. Nat Rev Cancer. 2022;22(4):195-207. doi:10.1038/s41568-022-00442-9.
- Tawbi H, Forsyth P, Algazi A. Combined nivolumab and ipilimumab in melanoma metastatic to the brain. N Engl J Med. 2018;379(8):722-730. doi:10.1056/NEJMoa1805453.
- Tawbi H, Forsyth P, Hodi F. Long-term outcomes of patients with active melanoma brain metastases treated with combination nivolumab plus ipilimumab (CheckMate 204): final results of an open-label, multicentre, phase 2 study. Lancet Oncol. 2021;22(12):1692-1704. doi:10.1016/S1470-2045(21)00545-3.
- Long G, Atkinson V, Lo S. Ipilimumab plus nivolumab versus nivolumab alone in patients with melanoma brain metastases (ABC): 7-year follow-up of a multicentre, open-label, randomised, phase 2 study. Lancet Oncol. 2025;26(3):320-330. doi:10.1016/S1470-2045(24)00735-6.
- A phase II, open-label, randomized, controlled trial of ipilimumab and nivolumab with concurrent intracranial stereotactic radiotherapy versus ipilimumab and nivolumab alone in patients with melanoma brain metastases. 2026.
- Carron R, Gaudy-Marqueste C, Amatore F. Stereotactic radiosurgery combined with anti-PD1 for the management of melanoma brain metastases: a retrospective study of safety and efficacy. Eur J Cancer. 2020;135:52-61. doi:10.1016/j.ejca.2020.04.028.
- Minniti G, Anzellini D, Reverberi C. Stereotactic radiosurgery combined with nivolumab or ipilimumab for patients with melanoma brain metastases: evaluation of brain control and toxicity. J Immunother Cancer. 2019;7(1):102. doi:10.1186/s40425-019-0588-y.
- Tang J, Mills M, Nakashima J. Clinical outcomes of melanoma brain metastases treated with nivolumab and ipilimumab alone versus nivolumab and ipilimumab with stereotactic radiosurgery. J Neurooncol. 2024;166(3):431-440. doi:10.1007/s11060-023-04543-9.
- Fu A, Bernstein K, Zhang J. Outcomes of concurrent versus non-concurrent immune checkpoint inhibition with stereotactic radiosurgery for melanoma brain metastases. J Neurooncol. 2025;173(3):619-625. doi:10.1007/s11060-025-05026-9.
- Messing I, Linkowski L, Riina M. Outcomes after SRS and ipilimumab plus nivolumab for melanoma brain metastases following prior immune checkpoint inhibitor or targeted therapy. Oncologist. 2026;31(4). doi:10.1093/oncolo/oyag043.
- Mandalà M, Amaral T, Rutkowski P. Combined immunotherapy with nivolumab and ipilimumab with and without sequential or concomitant stereotactic radiotherapy in patients with melanoma brain metastasis: an international retrospective study. Eur J Cancer. 2025;225. doi:10.1016/j.ejca.2025.115567.
- Altan M, Wang Y, Song J. Nivolumab and ipilimumab with concurrent stereotactic radiosurgery for intracranial metastases from non-small cell lung cancer: analysis of the safety cohort for non-randomized, open-label, phase I/II trial. J Immunother Cancer. 2023;11(7). doi:10.1136/jitc-2023-006871.
- Phase 1, 2 trial of concurrent anti-PD1 and stereotactic radiosurgery for melanoma and non-small cell lung cancer brain metastases (NCT02858869). 2026.
- Xu Y, Chen K, Xu Y. Brain radiotherapy combined with camrelizumab and platinum-doublet chemotherapy for previously untreated advanced non-small-cell lung cancer with brain metastases (C-brain): a multicentre, single-arm, phase 2 trial. Lancet Oncol. 2025;26(1):74-84. doi:10.1016/S1470-2045(24)00643-0.
- Li Y, Yu Q, Bu Q. First-line camrelizumab versus placebo plus chemotherapy with or without radiotherapy for brain metastases in NSCLC: the CTONG 2003 randomized placebo-controlled trial. J Thorac Oncol. 2025;20(7):928-940. doi:10.1016/j.jtho.2025.02.004.
- Schapira E, Hubbeling H, Yeap B. Improved overall survival and locoregional disease control with concurrent PD-1 pathway inhibitors and stereotactic radiosurgery for lung cancer patients with brain metastases. Int J Radiat Oncol Biol Phys. 2018;101(3):624-629. doi:10.1016/j.ijrobp.2018.02.175.
- Yomo S, Oda K, Oguchi K. Synergistic effects of immune checkpoint inhibitors in combination with stereotactic radiosurgery for patients with lung cancer and brain metastases: a propensity score-matched analysis. J Neurosurg. 2023;139(6):1628-1637. doi:10.3171/2023.4.JNS2349.
- Bashir S, Wen L, Zhang P. Efficacy and safety of combined immunotherapy and stereotactic radiosurgery in NSCLCBM patients and a novel prognostic nomogram: a real-world study. Front Oncol. 2023;13. doi:10.3389/fonc.2023.1068592.
- Shepard M, Xu Z, Donahue J. Stereotactic radiosurgery with and without checkpoint inhibition for patients with metastatic non-small cell lung cancer to the brain: a matched cohort study. J Neurosurg. 2020;133(3):685-692. doi:10.3171/2019.4.JNS19822.
- Singh C, Qian J, Yu J, Chiang V. Local tumor response and survival outcomes after combined stereotactic radiosurgery and immunotherapy in non-small cell lung cancer with brain metastases. J Neurosurg. 2020;132(2):512-517. doi:10.3171/2018.10.JNS181371.
- Singh S, McDermott D, Mattes M. Impact of systemic therapy type and timing on intracranial tumor control in patients with brain metastasis from non-small-cell lung cancer treated with stereotactic radiosurgery. World Neurosurg. 2020;144. doi:10.1016/j.wneu.2020.09.082.
- Scoccianti S, Olmetto E, Pinzi V. Immunotherapy in association with stereotactic radiotherapy for non-small cell lung cancer brain metastases: results from a multicentric retrospective study on behalf of AIRO. Neuro Oncol. 2021;23(10):1750-1764. doi:10.1093/neuonc/noab129.
- Dohm A, Tang J, Mills M. Clinical outcomes of non-small cell lung cancer brain metastases treated with stereotactic radiosurgery and immune checkpoint inhibitors, EGFR tyrosine kinase inhibitors, chemotherapy and immune checkpoint inhibitors, or chemotherapy alone. J Neurosurg. 2023;138(6):1600-1607. doi:10.3171/2022.9.JNS221896.
- Frehner L, Schär S, Hayoz S. First-line immunotherapy ± chemotherapy with or without upfront stereotactic radiotherapy (SRT) in patients with non-small cell lung cancer (NSCLC) with asymptomatic brain metastases. Lung Cancer. 2025;210. doi:10.1016/j.lungcan.2025.108813.
- Lu R, Wang Z, Tian W. A retrospective study of radiotherapy combined with immunotherapy for patients with baseline brain metastases from non-small cell lung cancer. Sci Rep. 2025;15(1):7036. doi:10.1038/s41598-025-91863-7.
- Chung J, Tos S, Mantziaris G. Stereotactic radiosurgery dose reduction for patients with brain metastases from non-small cell lung primary on immunotherapy or targeted therapy. Neurosurgery. 2026;12:10-1227. doi:10.1227/neu.0000000000003961.
- Flippot R, Dalban C, Laguerre B. Safety and efficacy of nivolumab in brain metastases from renal cell carcinoma: results of the GETUG-AFU 26 NIVOREN multicenter phase II study. JCO. 2019;37(23):2008-2016. doi:10.1200/JCO.18.02218.
- Emamekhoo H, Olsen M, Carthon B. Safety and efficacy of nivolumab plus ipilimumab in patients with advanced renal cell carcinoma with brain metastases: CheckMate 920. Cancer. 2022;128(5):966-974. doi:10.1002/cncr.34016.
- Hasanov E, Yeboa D, Tucker M. An interdisciplinary consensus on the management of brain metastases in patients with renal cell carcinoma. CA Cancer J Clin. 2022;72(5):454-489. doi:10.3322/caac.21729.
- Rathmell W, Rumble R, Van Veldhuizen P. Management of metastatic clear cell renal cell carcinoma: ASCO guideline. JCO. 2022;40(25):2957-2995. doi:10.1200/JCO.22.00868.
- Yomo S, Oda K, Oguchi K. Effectiveness of immune checkpoint inhibitors in combination with stereotactic radiosurgery for patients with brain metastases from renal cell carcinoma: inverse probability of treatment weighting using propensity scores. J Neurosurg. 2023;138(6):1591-1599. doi:10.3171/2022.9.JNS221215.
- Lehrer E, Gurewitz J, Bernstein K. Radiation necrosis in renal cell carcinoma brain metastases treated with checkpoint inhibitors and radiosurgery: an international multicenter study. Cancer. 2022;128(7):1429-1438. doi:10.1002/cncr.34087.
- Grant K, Gillespie Y, Karamian A. Evolving treatment paradigms for melanoma brain metastases: a systematic review of current modalities. Clin Neurol Neurosurg. 2025;257. doi:10.1016/j.clineuro.2025.109025.
- Williams G, Hong A, Thompson J. Treatment of melanoma brain metastases with radiation and immunotherapy or targeted therapy: a systematic review with meta-analysis. Crit Rev Oncol Hematol. 2024;202:104462. doi:10.1016/j.critrevonc.2024.104462.
- Li C, Li K, Zhong S. Which is the best treatment for melanoma brain metastases? A bayesian network meta-analysis and systematic review. Crit Rev Oncol Hematol. 2024;194:104227. doi:10.1016/j.critrevonc.2023.104227.
- Badrigilan S, Meola A, Chang S. Stereotactic radiosurgery with immune checkpoint inhibitors for brain metastases: a meta-analysis study. Br J Neurosurg. 2023;37(6):1533-1543. doi:10.1080/02688697.2021.2022098.
- Ahmadvand M, Habibi M, Mirjani M. The clinical outcomes of combined stereotactic radiosurgery with PD-1/PD-L1 inhibitors in patients with metastatic brain tumors: a systematic review and meta-analysis on the safety and efficacy. Neurosurg Rev. 2025;48(1). doi:10.1007/s10143-025-03909-z.
- Chu X, Niu L, Xiao G. The long-term and short-term efficacy of immunotherapy in non-small cell lung cancer patients with brain metastases: a systematic review and meta-analysis. Front Immunol. 2022;13. doi:10.3389/fimmu.2022.875488.
- Yang Y, Deng L, Yang Y. Efficacy and safety of combined brain radiotherapy and immunotherapy in non-small-cell lung cancer with brain metastases: a systematic review and meta-analysis. Clin Lung Cancer. 2022;23(2):95-107. doi:10.1016/j.cllc.2021.06.009.
- Taslimi S, Brar K, Ellenbogen Y. Comparative efficacy of systemic agents for brain metastases from non-small-cell lung cancer with an EGFR mutation/ALK rearrangement: a systematic review and network meta-analysis. Front Oncol. 2021;11. doi:10.3389/fonc.2021.739765.
- Gainor J, Shaw A, Sequist L. EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: a retrospective analysis. Clin Cancer Res. 2016;22(18):4585-4593. doi:10.1158/1078-0432.CCR-15-3101.
- Sneed P, Mendez J, Vemer-van den Hoek J. Adverse radiation effect after stereotactic radiosurgery for brain metastases: incidence, time course, and risk factors. J Neurosurg. 2015;123(2):373-386. doi:10.3171/2014.10.JNS141610.
- Minniti G, Scaringi C, Paolini S. Single-fraction versus multifraction (3 × 9 gy) stereotactic radiosurgery for large (>2 cm) brain metastases: a comparative analysis of local control and risk of radiation-induced brain necrosis. Int J Radiat Oncol Biol Phys. 2016;95(4):1142-1148. doi:10.1016/j.ijrobp.2016.03.013.
- Milano M, Grimm J, Niemierko A. Single- and multifraction stereotactic radiosurgery dose/volume tolerances of the brain. Int J Radiat Oncol Biol Phys. 2021;110(1):68-86. doi:10.1016/j.ijrobp.2020.08.013.
- Du G, Li W, Li J, Yu J, Zhu H. Concurrent immunotherapy is associated with increased radiation necrosis risk in lung cancer patients with brain metastases treated with stereotactic radiosurgery. Future Oncol. 2026;22(8):953-967. doi:10.1080/14796694.2026.2642933.
- Choi S, Hong A, Wang T. Risk of radiation necrosis after stereotactic radiosurgery for melanoma brain metastasis by anatomical location. Strahlenther Onkol. 2021;197(12):1104-1112. doi:10.1007/s00066-021-01798-x.
- Akhavan-Sigari A, Sbaih O, Hori Y. Perilesional edema as a predictor of local failure in metastatic brain lesions treated with stereotactic radiosurgery: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys. 2026;124(5):1199-1207. doi:10.1016/j.ijrobp.2025.06.3878.
- Ivanidze J, Shih R, Utukuri P. ACR appropriateness criteria® brain tumors. J Am Coll Radiol. 2025;22(5s):S108-S135. doi:10.1016/j.jacr.2025.02.036.
- Alexander B, Brown P, Ahluwalia M. Clinical trial design for local therapies for brain metastases: a guideline by the response assessment in neuro-oncology brain metastases working group. Lancet Oncol. 2018;19(1). doi:10.1016/S1470-2045(17)30692-7.
- Govaerts C, Kramer M, Bosma I. Incidence and clinical features of pseudoprogression in brain metastases after immune-checkpoint inhibitor therapy: a retrospective study. Cancers. 2025;17(15). doi:10.3390/cancers17152425.
- Park H, Kim K, Pyo J. Incidence of pseudoprogression during immune checkpoint inhibitor therapy for solid tumors: a systematic review and meta-analysis. Radiology. 2020;297(1):87-96. doi:10.1148/radiol.2020200443.
- Chuang M, Liu Y, Tsai Y, Chen Y, Wang C. Differentiating radiation-induced necrosis from recurrent brain tumor using MR perfusion and spectroscopy: a meta-analysis. PLoS One. 2016;11(1). doi:10.1371/journal.pone.0141438.
- Okada H, Weller M, Huang R. Immunotherapy response assessment in neuro-oncology: a report of the RANO working group. Lancet Oncol. 2015;16(15). doi:10.1016/S1470-2045(15)00088-1.
- Yu J, Zheng J, Xu W. Accuracy off-FDOPA positron emission tomography andf-FET positron emission tomography for differentiating radiation necrosis from brain tumor recurrence 18 18. World Neurosurg. 2018;114. doi:10.1016/j.wneu.2018.03.179.
- Zhou C, Kou Y, Zhou W. Diagnostic value of PET tracers in differentiating glioma tumor recurrence from treatment-related changes: a systematic review and meta-analysis. AJNR Am J Neuroradiol. 2025;46(4):758-765. doi:10.3174/ajnr.A8565.
- Vellayappan B, Lim-Fat M, Kotecha R. A systematic review informing the management of symptomatic brain radiation necrosis after stereotactic radiosurgery and international stereotactic radiosurgery society recommendations. Int J Radiat Oncol Biol Phys. 2024;118(1):14-28. doi:10.1016/j.ijrobp.2023.07.015.
- Xu Y, Rong X, Hu W. Bevacizumab monotherapy reduces radiation-induced brain necrosis in nasopharyngeal carcinoma patients: a randomized controlled trial. Int J Radiat Oncol Biol Phys. 2018;101(5):1087-1095. doi:10.1016/j.ijrobp.2018.04.068.
- Nobel H, Ofer J, Borenstein S. Long-term impact of bevacizumab for the treatment of brain radiation necrosis. J Neurooncol. 2025;173(2):289-296. doi:10.1007/s11060-025-04979-1.
- Upadhyay R, Elguindy A, Salts L. Boswellia serrata for cerebral radiation necrosis after radiosurgery for brain metastases. Int J Radiat Oncol Biol Phys. 2025;122(5):1282-1291. doi:10.1016/j.ijrobp.2025.02.016.
- Sankey E, Grabowski M, Srinivasan E. Time to steroid independence after laser interstitial thermal therapy vs medical management for treatment of biopsy-proven radiation necrosis secondary to stereotactic radiosurgery for brain metastasis. Neurosurgery. 2022;90(6):684-690. doi:10.1227/neu.0000000000001922.
- Palmisciano P, Haider A, Nwagwu C. Bevacizumab vs laser interstitial thermal therapy in cerebral radiation necrosis from brain metastases: a systematic review and meta-analysis. J Neurooncol. 2021;154(1):13-23. doi:10.1007/s11060-021-03802-x.
- Lehrer E, Peterson J, Zaorsky N. Single versus multifraction stereotactic radiosurgery for large brain metastases: an international meta-analysis of 24 trials. Int J Radiat Oncol Biol Phys. 2019;103(3):618-630. doi:10.1016/j.ijrobp.2018.10.038.
- Jessurun C, Hulsbergen A, de Wit A. The combined use of steroids and immune checkpoint inhibitors in brain metastasis patients: a systematic review and meta-analysis. Neuro Oncol. 2021;23(8):1261-1272. doi:10.1093/neuonc/noab046.
- Yomo S, Oda K, Oguchi K. Pre-stereotactic radiosurgery neutrophil-to-lymphocyte ratio predicts post-stereotactic radiosurgery survival of patients with brain metastases concurrently treated with immune checkpoint inhibitors. J Neurosurg. 2025;142(2):454-463. doi:10.3171/2024.5.JNS24259.
- Tracz J, Donnelly B, Ngu S. The abscopal effect: inducing immunogenicity in the treatment of brain metastases secondary to lung cancer and melanoma. J Neurooncol. 2023;163(1):1-14. doi:10.1007/s11060-023-04312-8.
- Levy A, Massard C, Michiels S, Deutsch E. Innovative, early-phase clinical trials of drug-radiotherapy combinations. Lancet Oncol. 2025;26(4). doi:10.1016/S1470-2045(24)00664-8.
- Bhatti N, Young D, Lam W. Attention-guided deep learning of chemical exchange saturation transfer magnetic resonance imaging to differentiate between tumor progression and radiation necrosis in brain metastasis. Int J Radiat Oncol Biol Phys. 2026;125(2):630-641. doi:10.1016/j.ijrobp.2025.10.040.
- Yu Y, Luo Y, Zeng F, Liu A. Opportunities and challenges for non-small cell lung cancer brain metastases in the immunotherapy era. Cancer Treat Rev. 2025;140:103014. doi:10.1016/j.ctrv.2025.103014.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Acknowledgments
The author used ChatGPT (OpenAI) to assist with language editing and manuscript refinement. All content was reviewed and verified by the author for accuracy.
Citation
. Stereotactic Radiosurgery and Immunotherapy for Melanoma and NSCLC Brain Metastases: Practical Integration, Timing, and Toxicity. Applied Radiation Oncology. 2026;15(2). doi:10.37549/ARO-D-26-0008.