Getting Personal: Optimizing RT Dosing Strategies for Improved Outcomes
Images
With the goal of destroying cancer while minimizing harm, considering each patient’s specific tumor biology enables multidisciplinary care teams to improve tumor control while minimizing toxicity. Using genomics, radiomics, and personalized medicine, researchers at Florida-based Moffitt Cancer Center are investigating ways to identify target areas based on radiosensitivity within sarcomas and breast cancers to improve personalized care through altered fractionation of RT delivery.
“Utilizing dose painting and hypofractionation is a very easy next step forward,” says Arash Naghavi, MD, associate professor of radiation oncology, section head for sarcoma, and brachytherapy fellowship program director at Moffitt Cancer Center, who has been implementing the treatment methods in patient care.
While surgery remains the gold standard for sarcoma treatment, dose painting enables pre-operative delivery of non-uniform radiation dosing to the clinical target for patients at a high risk of recurrence. For breast cancer, researchers are integrating a genomic biomarker predictive of radiosensitivity, the radiosensitivity index (RSI), into the linear quadratic model to derive the optimal genomic-adjusted radiation dose, or GARD, for the target.1
“GARD has been validated for multiple primary histologies including glioblastoma, pancreatic cancer, lung tumors, and breast cancer as a predictive biomarker specifically for radiation therapy benefit,” explains Matthew Mills, MD, assistant member of the department of radiation oncology at Moffitt Cancer Center.
In breast cancer care, GARD is associated with local control following postsurgical RT; in treatment of sarcoma, researchers have found that hypofractionation can improve disease control without a significant difference in long-term toxicity.
“A one-size-fits-all approach to dosing is likely not appropriate. RSI/GARD tools can be used to personalize radiation dose based on the unique genomic profile of the tumor,” explains Kamran Ahmed, MD, section chief of breast radiation oncology and associate member of the department of radiation oncology at Moffitt.
Dose Painting, Hypofractionation, and Novel Strategies in Sarcoma Treatment
Treatment of soft-tissue sarcoma, comprised of more than 50 different subtypes, requires an approach that addresses this heterogeneity since conventional, standard RT doses tend to yield nonuniform responses.
“Some areas of a person’s tumor are more aggressive. In traditional dosing of 2 Gy per fraction, we found that really it’s not that [sarcomas] are radioresistant, we may just not have found the right dose yet to get them to respond,” says Dr. Naghavi.
Genomically, Moffitt researchers identified sarcoma’s low alpha/beta (a/b) ratio, the proportion of its sensitivity to radiation, and how it’s able to overcome the effects of radiation. Delivering a higher dose per fraction, or hypofractionation, to a large sarcoma can help overcome its ability to repair between treatments. Considering the risks of long-term toxicity, the researchers sought to determine whether they could selectively dose escalate with hypofractionation to the areas at highest risk, while maintaining normal to lower doses in non-high-risk areas.
“Hypofractionation is slowly being implemented for different disease processes because it has a more profound effect on cells that have a low a/b like melanoma, prostate, breast cancer and sarcoma, where they’re able to repair DNA damage between standard radiation fractions, and the higher dose per day overcomes this repair,” Dr. Naghavi explains.
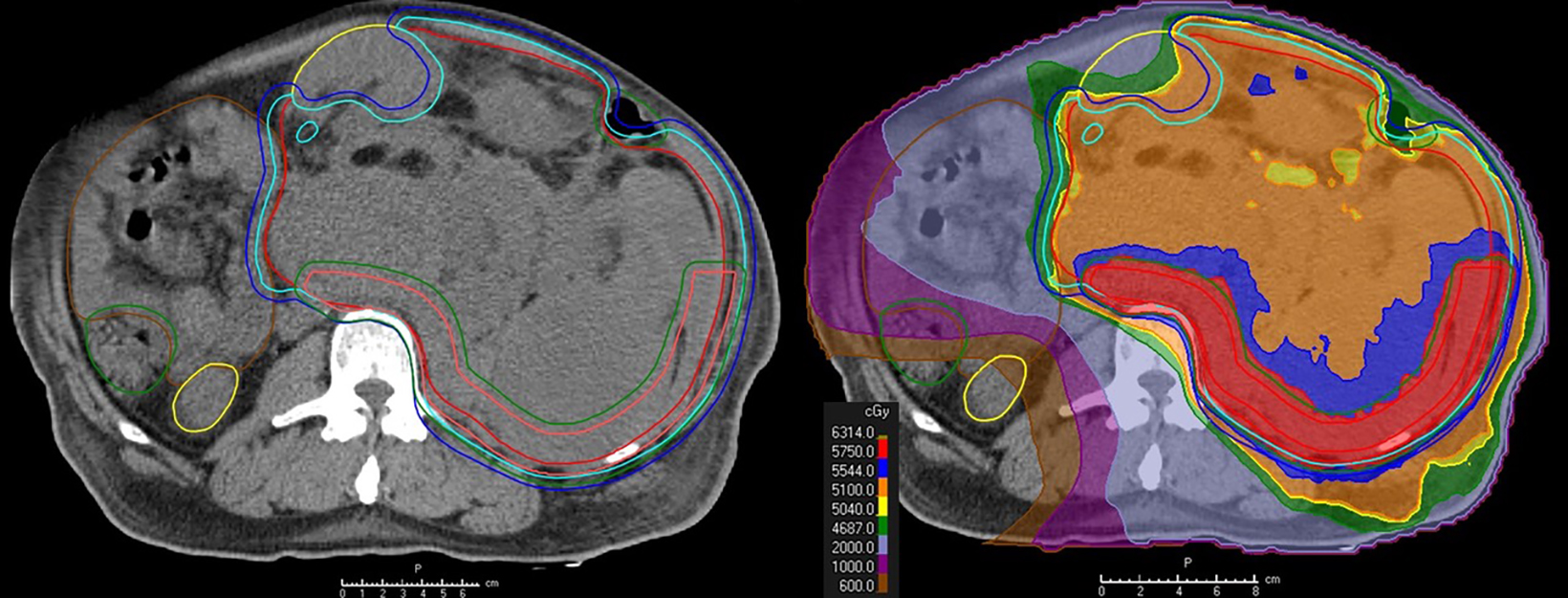
Dose painting, or simultaneous integrated boost, uses dosimetric techniques to “paint” the areas requiring higher doses, allowing treatment teams to escalate dose safely rather than giving a blanketed higher dose over the whole area, which contributes to toxicity. This strategy has been effective in treating retroperitoneal sarcoma, where clear margins in surgery are often difficult.2 (Figure 1)
An illustration of the retroperitoneal sarcoma study.2 The area at highest risk of microscopic disease is escalated after surgery. The area that is the most difficult to resect and has the highest risk of disease is posterior, next to blood vessels and paravertebral, while the area abutting the bowel and kidney get a standard dose.
“To improve control, we increase the dose where we know surgeons are going to have trouble…accounting for the areas that have the highest risk of microscopic cells being left behind,” Dr. Naghavi explains, noting that 5-year control was improved by 26%. “There is correlation between the response to preoperative treatment and patient outcome, so if you can get the tumor to respond really well before surgery, there’s an improved chance of them being able to get it all out, and improving local control, distant control, progression-free survival, and overall survival.”
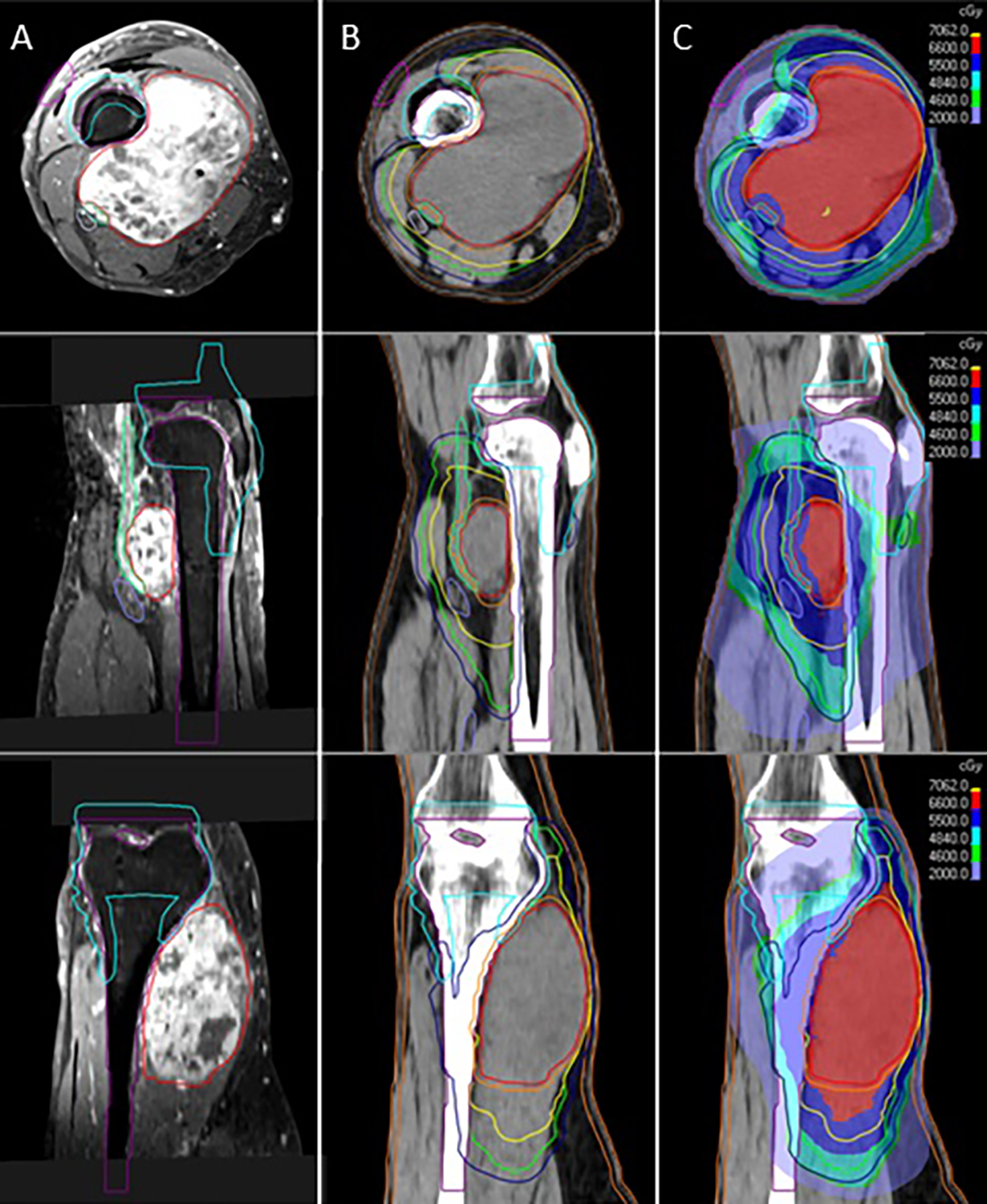
In unresectable sarcoma patients, Dr. Naghavi uses an approach called Hypofractionated Accelerated Radiation Dose-Painting (HARD),3 which he presented on at ASTRO. Visualizing the gross tumor volume on a T1-postcontrast MRI, the cell density of cancers is identifiable, including the highest density area and less dense areas beyond the pseudocapsule in the clinical target volume. The lower-risk areas are treated with standard dosing of 1.8 to 2 Gy per fraction, with dose painting through hypofractionation of 2.5 to 3 Gy. (Figure 2)
“The area getting dialed up is the area of highest risk…Using this approach, we’re able to delineate the target and escalate safely,” Dr. Naghavi says, protecting adjacent organs at risk.
“We found that the standard fractionation [2 Gy per day] had 59% locoregional control at 2 years, which is consistent with the literature, but that HARD had a 96% locoregional control, which is a >36% improvement. HARD independently predicted for locoregional control, without a significant difference in late grade 3 toxicity (~6% to 7%),” Dr. Naghavi reports, offering an option to patients with unresectable tumors with no worse toxicity than standard radiation.
Further, when examining the estimated cost of the HARD technique—through eliminating between 4 and 7 fractions of RT—the researchers determined that they were saving $2,700 to $4,400 per patient.3
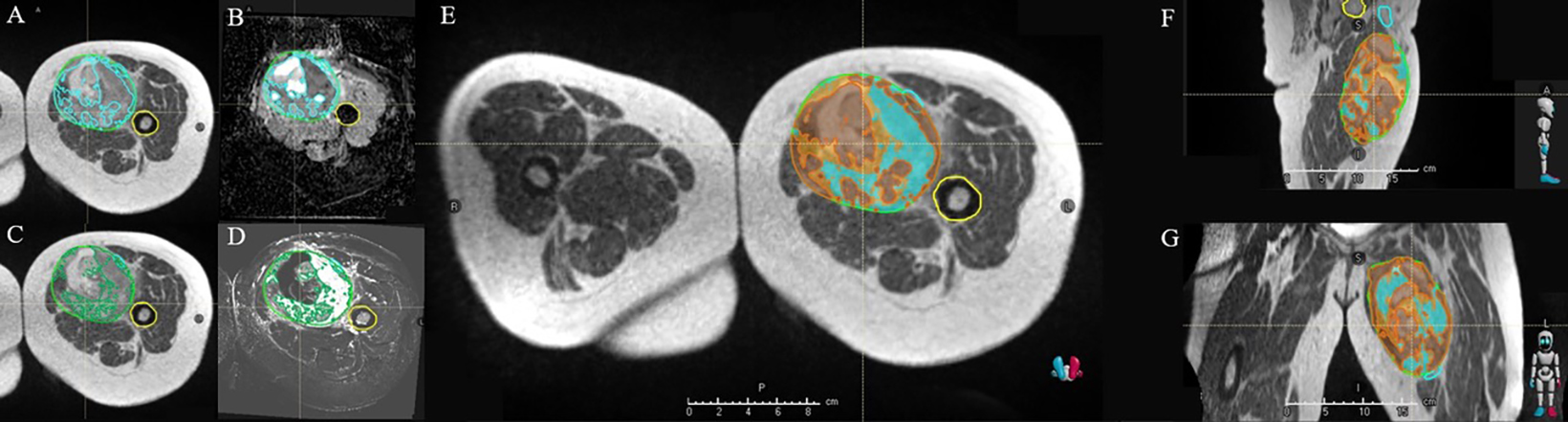
Similarly, in the Habitat Escalated Adaptive Radiotherapy trial (HEAT),4 Moffitt researchers are using radiomic habitats—overlayed MR imaging that identifies subpopulations within the tumor, which represent the innate biology—to identify hypoxic and cell-dense areas, giving them a targeted strike with focal hypofractionated radiation dose escalation utilizing simultaneous integrated boost. The HEAT method provides a means to improve response, impacting disease control locally and distantly, by identifying subcomponents within the tumor that may be orchestrating progression. Based on the genetic radiosensitivity of sarcoma in 231 patients, researchers were able to estimate the probability of response by the dose received. (Figure 3)
This is the first trial to use genetics to design a personalized radiation framework for patients, and is the first to utilize radiomic habitats to focally dose-escalate with hypofractionation. According to Dr. Naghavi, preliminary results have been astounding, with one of the highest reported pathologic response rates known to date.
“The cookie-cutter way we’ve been treating sarcoma has been all wrong,” Dr. Naghavi reports. “A genomically and radiomically personalized approach allows us to safely dose-escalate sarcoma, forcing a paradigm shift in the way it’s radiated.”
On GARD: Personalizing Breast Cancer Care
Similar to sarcoma, breast cancer cells have a low a/b, making the site optimal for hypofractionation. Divergently, radiation approaches are much more standardized in the breast, with extensive data guiding multiple adjuvant hypofractionation regimens with a concomitant or sequential boost postsurgery. Moffitt researchers are personalizing breast care using genomics, an area of promise for disease treatment.
Using the RSI model based on 10 specific genes, researchers are predicting radiosensitivity for each specific tumor, something that was once estimated on averages. While they found that the RSI usually agreed with the generally understood radiosensitivity for a primary tumor, there was important heterogeneity across tumors within a particular primary diagnosis.
“Matching the treatment to that radiosensitivity seemed like an opportunity to improve personalized care,” says Dr. Mills.
In their first application of GARD into triple-negative breast cancer, researchers found that GARD was a significant predictor of local control in 2 independent cohorts.1
“We found that we could utilize GARD to try to calculate which individualized radiation dose would be required for each patient to optimize their therapy based on their own specific tumor’s radiosensitivity,” Dr. Mills explains, noting that at 50 Gy, half the patients were already optimized and could be spared the 10 Gy boost that was standardly given.
A trial is underway examining the use of RSI to determine whether triple negative breast cancer patients receive a boost or not based on their unique RSI.5
Researchers continue to focus on identifying the optimal means of delivering RT on an individual patient level.
The Future
Investigations and applications of genomic analyses are advancing not only at Moffitt, but nationwide, to inform better radiation decisions.
“Our phase II study of radiation dose personalization for the adjuvant management of triple negative breast cancer following lumpectomy using RSI is an initial step to validate the use of RSI in breast cancer management,” says Dr. Ahmed. “There are other genomic signatures like the Oncotype DX score being used in the TAILOR RT study6 to modify radiation fields for breast cancer. A multitude of dose/fractionation strategies are available for breast cancer and genomics that may help us identify the appropriate radiation dose and targets for each patient.”
“In breast cancer, it’s often about treating patients just enough and not any more than that,” Dr. Mills adds, continuing “so really finding biomarkers to accurately estimate a given patient’s risk of recurrence is key. We have to be able to identify patents who would benefit from adjuvant radiation and those who can safely avoid it. This is where the field is moving.”
Dr. Mills’ team is interested in a dose-escalation trial using MR-guided radiation therapy for added precision, potentially increasing doses as well as the interval between RT and therapy to increase response. Doing so utilizing RSI is another future direction, he says.
Dr. Naghavi notes that trials like HEAT will inform how treatment teams escalate dose not only based on concentration of cancer cells, but by identifying exactly how sensitive a tumor is in various areas. Bigger picture, he predicts evolving paradigms in cancer care, adding that sarcoma is the perfect starting point.
“One day, based off of imaging alone, I could tell you what the biology of your tumor and the genetics look like, what target agents or chemotherapies your tumor would respond to, and what your outcome would be, without ever doing a biopsy. That’s what we’re hoping to achieve,” Dr. Naghavi concludes. “With sarcoma, you’re starting with a basket full of these different histologies where you have to get creative to personalize treatment. With a blanketed treatment, you’ll never get the answers you’re looking for.”
References
- Ahmed KA, Liveringhouse CL, Mills MN, et al. Utilizing the genomically adjusted radiation dose (GARD) to personalize adjuvant radiotherapy in triple negative breast cancer management. EBioMedicine. 2019;47:163-169. doi: 10.1016/j.ebiom.2019.08.019. Epub 2019 Aug 12. PMID: 31416721; PMCID: PMC6796536
- Liveringhouse CL, Palm RF, Bryant JM, et al. Neoadjuvant simultaneous integrated boost radiation therapy improves clinical outcomes for retroperitoneal sarcoma. Int J Radiat Oncol Biol Phys. 2023;117(1)123-138. ISSN 0360-3016, https://doi.org/10.1016/j.ijrobp.2023.03.037
- Mills MN, Liveringhouse C, Brant JM, Yang GQ, Naghavi AO. Novel hypofractionated accelerated radiotherapy dose (HARD) utilizing simultaneous integrated for unresectable soft tissue sarcomas. Int J Radiat Oncol Biol Phys. 2022:114(3), e609.https://doi.org/10.1016/j.ijrobp.2022.07.1818
- Habitat Escalated Adaptive Therapy (HEAT), With Neoadjuvant Radiation for Soft Tissue Sarcoma. H. Lee Moffitt Cancer Center and Research Institute, accessed viahttps://classic.clinicaltrials.gov/ct2/show/NCT05301283
- Genomically Guided Radiation Therapy in the Management of Triple Negative Breast Cancer. H. Lee Moffitt Cancer Center and Research Institute, accessed via https://classic.clinicaltrials.gov/ct2/show/NCT05528133
- Regional Radiotherapy in Biomarker Low-Risk Node Positive and T3N0 Breast Cancer (TAILOR RT). Canadian Cancer Trials Group, accessed via https://clinicaltrials.gov/study/NCT03488693