Volumetric-modulated arc therapy improved heart and lung sparing for a left-sided chest wall and regional nodal irradiation case
Images


CASE SUMMARY
A 56-year-old postmenopausal woman initially presented in October 2013 with complaints of intermittent left breast pain, redness and a left axillary mass for several months. Clinical examination was notable for an edematous and erythematous left breast with peau d’orange and a palpable underlying 6-cm mass with bulky axillary lymphadenopathy. Core biopsies of the left breast and left axilla demonstrated poorly differentiated ductal carcinoma, ER-/PR-/Her2-. Skin biopsy was negative. Workup was negative for metastatic disease, and the cancer was staged IIIB cT4d N2a M0. Beginning in December 2013, the patient was treated with neoadjuvant chemotherapy consisting of 4 cycles of dose dense Adriamycin and cyclophosphamide (AC) followed by Taxol and carboplatin (TC), which consisted of 12 cycles of Taxol and 3 cycles of carboplatin (the last dose of carboplatin was held due to electrolyte wasting). Genetic testing was positive for BRCA2 mutation. The patient subsequently developed an Adriamycin-related cardiomyopathy in which her ventricular ejection fraction dropped from 65% to 45% and did not recover. The patient underwent left modified radical mastectomy and prophylactic right mastectomy in June 2014. There was no residual carcinoma in the left breast. Four of 16 axillary lymph nodes contained metastatic disease. The patient then presented in July 2014 for postmastectomy radiation therapy (PMRT).
IMAGING, PATHOLOGY FINDINGS
A bilateral mammography in October 2013 showed bulky left axillary adenopathy, some of which was associated with heterogeneous microcalcifications, extensive skin thickening, and a 2-cm area of pleomorphic calcifications in the upper outer quadrant of the breast corresponding to the marked palpable abnormality. On ultrasound, diffuse skin thickening was seen throughout the left breast. There were large confluent areas of irregular marginated hypoechoic tissue in the upper outer quadrant and multiple abnormal axillary lymph nodes containing calcification. The patient underwent ultrasound-guided biopsy of the left breast lesion in the 2:30 axis and 7 cm from the nipple, and of an enlarged left axillary lymph node. Pathology from the left breast demonstrated infiltrating poorly differentiated ductal carcinoma and focal intermediate grade ductal carcinoma in situ (DCIS), solid type, ER-/PR-/Her2-. The left axillary lymph node contained poorly differentiated infiltrating ductal carcinoma with associated necrosis and calcifications. Punch biopsy of the skin showed chronic inflammation of the dermis. Bilateral breast MRI was performed in November 2013 before initiating neoadjuvant chemotherapy. In the left breast, there was generalized skin thickening, an irregular heterogeneously enhancing mass and nonmass enhancement throughout the entire lateral breast (10 × 10 × 6.4 cm) extending into the pectoralis muscle, with associated tethering and irregularity of the pectoralis fascia (no enhancement of pectoralis muscle), an abnormal subpectoral lymph node (1.5 cm), and bulky left axillary adenopathy with the largest lymph node (4 × 2.5 × 2.5 cm in diameter). No adenopathy of the internal mammary nodes (IMNs) was seen. Following chemotherapy, a bilateral breast MRI (May 2014) demonstrated near-complete resolution of the extensive enhancement in the left breast and complete resolution of left axillary adenopathy. No suspicious findings were noted in the right breast. Bilateral mammogram and ultrasound in May 2014 demonstrated in the left breast 2 new groups of suspicious pleomorphic microcalcifications in the upper outer quadrant. Biopsy of these microcalcifications was not performed as the patient elected to proceed with bilateral mastectomy.
The patient underwent left modified radical mastectomy and prophylactic right mastectomy. Pathology of the left mastectomy specimen demonstrated no residual carcinoma in the left breast. There was lobular carcinoma in situ with atypical lobular hyperplasia, florid duct hyperplasia, radial scar, fibrocystic changes and associated calcifications. Skin, nipple and deep margin were negative. Residual carcinoma was identified in 4 out of 16 left axillary lymph nodes with therapy-related changes, the largest measuring 1 cm, without extracapsular extension, ER-/PR-/Her2- on immunohistochemistry and fluorescence in situ hybridization.
DIAGNOSIS
The patient presented with inflammatory breast cancer (IBC) and the diagnosis was based on the initial clinical breast examination, which is defined by erythema, edema and peau d’orange. The patient was clinically staged IIIB (cT4d N2a M0); morphology of infiltrating poorly differentiated ductal carcinoma, ER-/PR-/Her2-. She underwent neoadjuvant chemotherapy with a partial radiographic and pathologic response. However, there was residual disease in the axilla (macrometastases). Given her age, pathologic findings, and the aggressive nature of triple negative inflammatory breast cancer, postmastectomy radiation treatment was clearly indicated.
LITERATURE REVIEW
A retrospective analysis of 316 patients with IBC who received trimodality therapy consisting of neoadjuvant chemotherapy, modified radical mastectomy and postmastectomy radiation to the chest wall and regional lymph nodes, has shown that of all 4 subtypes of breast cancer (ER+/PR+/HER2+, ER+/PR+/HER2-, ER-/PR-/HER2+, ER-/PR-/HER2-), triple negative (TN/ ER-/PR-/HER2-) breast cancer is associated with higher rates of distant relapse (DR), locoregional recurrence (LRR) and worse overall survival (OS).1 The median OS time was 40 months for the ER+/PR+/HER2+ subtype, 38 months for ER+, 29 months for HER2+ and 24 months for the TN subtype. The median time to LRR was 35 months for the ER+/PR+/HER2+ subtype, 36 months for ER+, 26 months for HER2+ and 19 months for the TN subtype. The median time to DR was 31 months for ER+/PR+/HER2+, 34 months for ER+, 22 months for the HER2+ group and 19 months for the TN subtype, which, therefore, remains a therapeutic challenge.
The risk of LRR is a greater concern in patients with IBC especially in the triple negative (TN) subtype.1 Patients with IBC undergoing trimodality therapy who received neoadjuvant therapy were more likely to have residual disease in the axilla increasing their risk for locoregional recurrence, further emphasizing the need for optimal regional nodal management.2 Moreover, a large percentage of locoregional failures had a regional component.2 A nonrandomized study found that accelerated hyperfractionated radiation therapy (RT) to a total dose of 66 Gy at 1.5 Gy per fraction delivered twice daily [vs.] 60 Gy at 2 Gy per fraction delivered once daily had better local control for IBC.3 The study also showed that among patients who were treated twice a day to a total dose of 66 Gy vs. 60 Gy, the locoregional control (LRC) at 5 years was 84.3% vs. 57.8%, and at 10 years was 77% vs. 57.8%. A 3- to 5-mm thick bolus (tissue equivalent material) was used to increase dose to the skin/superficial tissue for every fraction during the first week, followed by only the first fraction of the day for the second week, and then as needed for the remaining treatment. However, as shown by a study from MD Anderson, this accelerated hyperfractionation regimen increased skin toxicity.4 The LRR rate in patients treated after 1994 (when taxanes were introduced as adjuvant therapy) was 8% for a total dose of 66 Gy. Bolus of 3-5 mm thickness was placed on the chest wall with the same frequency described earlier.3 The rate of late skin toxicity among patients treated to a total dose of 66 Gy was almost twice as large at 29% compared to 15% among those treated to a total dose of 60 Gy.4 This study led to the recommendation that escalation of postmastectomy radiation dose to 66 Gy appeared to only benefit patients with poor response to chemotherapy and those who were < 45 years old. Patients > 45 years old and who had achieved good response to neoadjuvant chemotherapy should be treated with conventional fractionation. In this respect, a later study from Memorial Sloan Kettering Cancer Center (MSKCC) reported that in patients treated to a total dose of 50 Gy to the chest wall and regional lymph nodes in daily fractions of 1.8 Gy or 2 Gy with skin bolus of thickness 0.5 cm – 1 cm applied over the chest wall for each fraction, had a LRR rate of 13%,5 which is slightly higher than that reported from MD Anderson.4 These patients were treated after 1995, had received taxanes as part of their combined modality therapy and the majority of them (89%) did not receive a scar boost. In our case, our patient was > 45 years of age, had received a taxane and had no residual disease in the breast following neoadjuvant chemotherapy. However, since she had 4 out of 16 axillary lymph nodes containing metastatic disease, adequate coverage of the regional lymph nodes was essential.2 Therefore, a course of adjuvant postmastectomy radiation therapy to the left chest wall, axilla, supraclavicular fossa, and internal mammary nodes (IMNs) was recommended to 50.4 Gy in 1.8 Gy fractions delivered once daily along with a 5-mm thick bolus covering the chest wall for each fraction.
Including IMNs during irradiation of the left breast is known to increase dose exposure to the underlying normal tissue such as the heart and lung. This patient had exposure to Adriamycin and she suffered from cardiomyopathy having a left ventricular ejection fraction of 45%. Cyclophosphamide is known to cause pulmonary toxicity by local inflammation in the lung parenchyma affecting gas exchange,6 potentially exacerbating lung injury caused by RT. The risk of radiation pneumonitis (RP) post RT in patients who have received chemotherapy with taxanes is also a concern.7 Given this patient’s risk factors for cardiopulmonary toxicities, the heart and the lung dose had to be minimized as much as possible while providing adequate radiation dose to the left chest wall and regional lymph nodes.
TREATMENT PLANNING TECHNIQUES
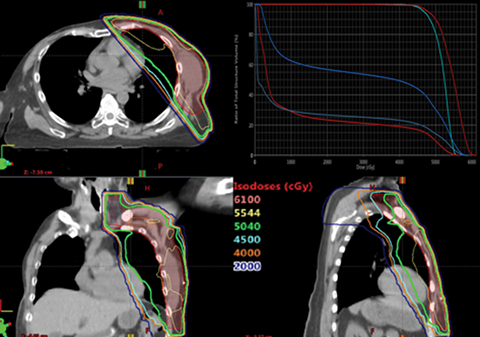
The partially wide tangents (PWT) technique is considered the most appropriate balance of target coverage and normal tissue sparing8,9 and was initially used to plan this case. Details on patient simulation and contouring have been described earlier.10,11 The dose distribution with the PWT plan is shown in Figure 1. The amount of lung incorporated with this technique was > 3 cm, the resulting mean heart dose (MHD) was 13.6 Gy, and the ipsilateral lung V20 Gy was 56.9%. Darby et al have shown that the rate of a major coronary event increases linearly by 7.4% per Gy of MHD.12 Moreover, women with preexisting cardiac risk factors have a higher increase in the absolute risk than women without these factors. Therefore, there was a need to reduce the MHD for this case to as low as can be achieved. Short-term pulmonary side effects in breast cancer patients after adjuvant RT showed no cases of RP in patients whose ipsilateral lung V20 Gy was kept at < 30%,13 while exceeding this constraint increased the likelihood of pulmonary complications.14 Since cardiopulmonary toxicity was a concern in this case, given the dosimetric parameters, the PWT technique was unable to provide a viable plan for treatment.
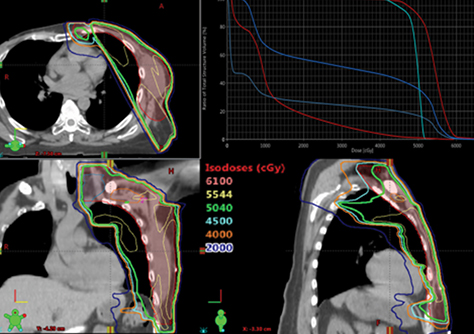
The depth of heart and lung included in the tangential fields can impact the volumetric doses and, therefore, it has been shown that a combination of photons and electrons can reduce the heart and lung doses, especially over the use of tangential fields when the depth of the lung treated is > 3 cm.15 Two photon/electron (P/E) techniques were then planned, namely the 20/80 photon/electron mix and the 30/70 photon/electron mix8,15 with 6 MV photons and 12 MeV electrons. The MHD was comparable with both P/E techniques (12.4 Gy vs. 12.1 Gy, respectively); however, the MILD with the former was slightly lower at 31.2 Gy compared to 32.7 Gy, as was the V20 Gy (56.8% vs. 60.8%). Figure 2 displays the dose distribution for the 20/80 photon/electron mix. Although the MHD was comparable among the two techniques, no benefit was seen with the 20/80 photon/electron mix in reducing dose to the ipsilateral lung over PWT.
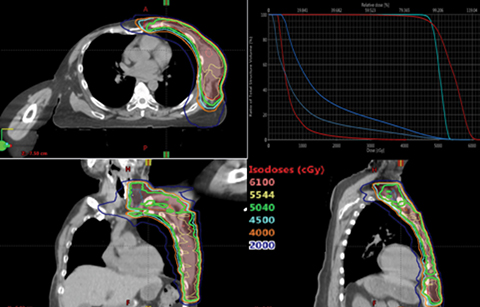
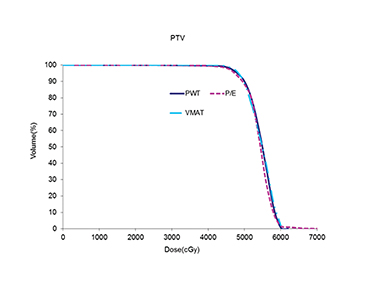
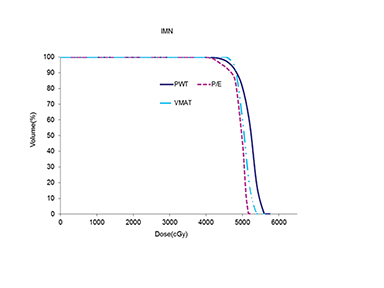
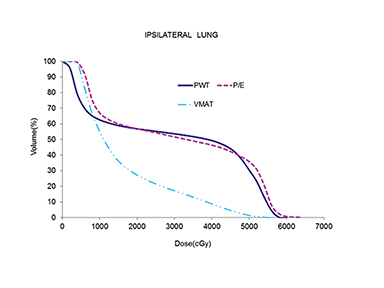
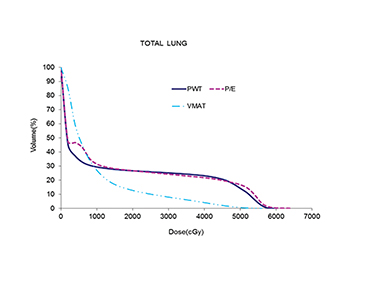
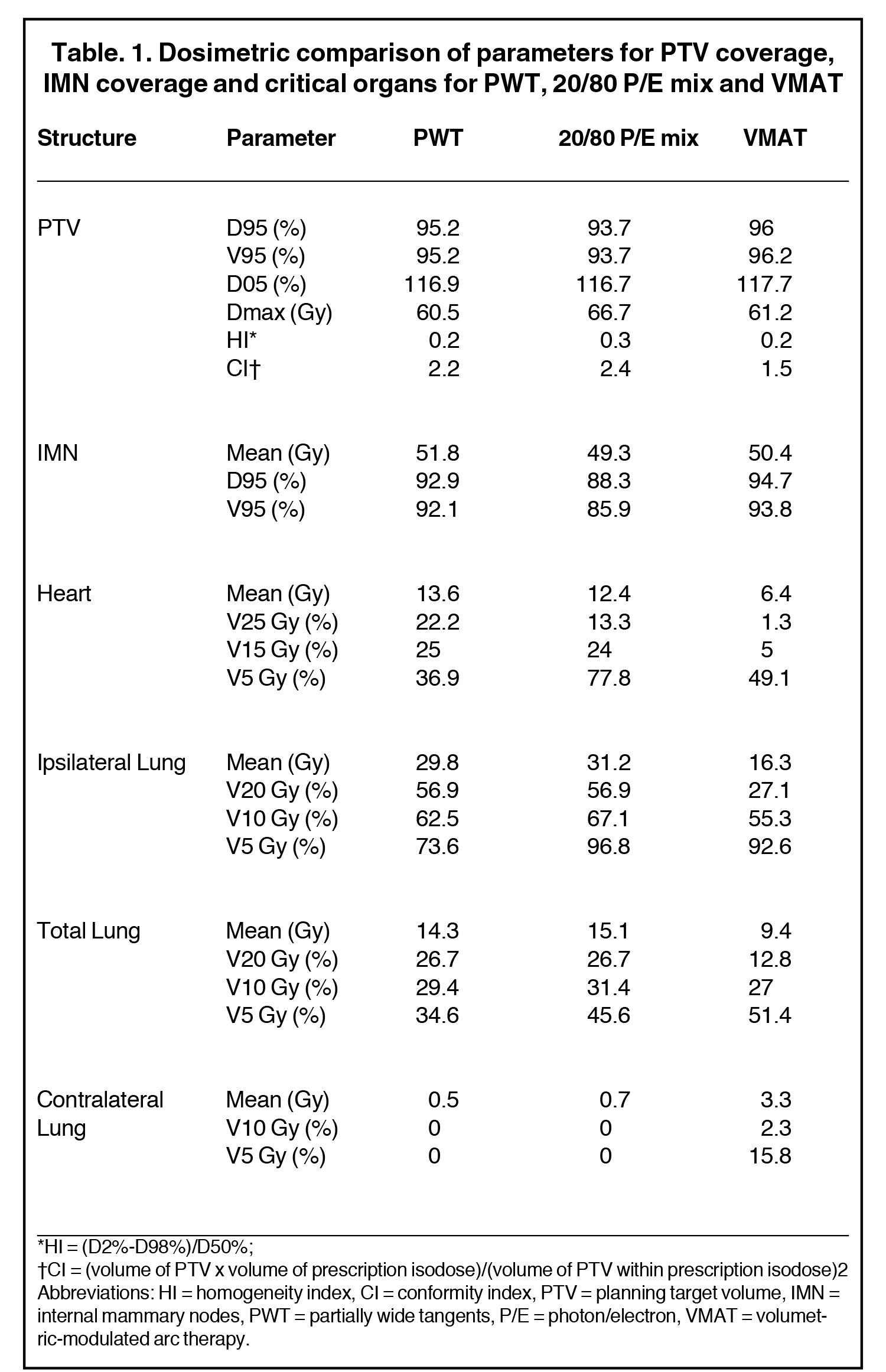
The use of multibeam intensity-modulated radiation therapy (IMRT) or volumetric-modulated radiation therapy (VMAT) in such situations can help improve target coverage, conformity and homogeneity while sparing the heart and lung from doses ≥ 15 Gy.16-18 This approach is known to carve out high-dose areas around the heart, specifically related to the coronary arteries. We then planned this case with VMAT using 2 partial coplanar arcs of range 210° (from 300° to 150°). Details of the field arrangement and planning have been published earlier10 and we closely followed those described by Popescu et al.18 Dose distribution for the VMAT plan is shown in Figure 3. The definition of homogeneity index (HI) and conformity index (CI) are the same as in our previous case report.19 Compared to both 3DCRT planning techniques, the MHD with VMAT was reduced by almost 50% to 6.4 Gy. VMAT also reduced the mean ipsilateral lung dose (MILD) to 16.3 Gy and the V20 Gy to 27.2%. Comparison of the DVHs for the 3 plans is shown in Figure 4, which illustrates the superior heart and lung sparing and adequate coverage achieved with VMAT compared to PWT and 20/80 photon/electron mix techniques. Table 1 shows a detailed dosimetric comparison of the various dosimetric parameters amongst the different planning techniques. Contouring of the chest wall clinical target volume (CTV) and the nodal CTV was done as per the Radiation Therapy Oncology Group (RTOG) breast cancer contouring atlas.20 The planning target volume (PTV) was CTV + 5 mm margin and included the skin in the chest wall region. For a uniform basis of comparison, the PTV was kept the same in all plans.
DISCUSSION
Exposure of the heart to ionizing radiation during RT of the left breast/chest wall is unavoidable and depends on the patient’s anatomy.18 It is known to increase a patient’s long-term risk of developing ischemic heart disease.12 This increase is proportional to the MHD, and women with preexisting cardiac risk factors have an even greater absolute increase in risk from radiation. The absolute risk for a 56-year-old patient who received an MHD of 6 Gy with at least 1 existing cardiac risk factor of suffering from an acute coronary event (nonfatal or fatal major coronary event [MCE], or unstable angina) within the first 10 years after receiving radiation is 2% to 3.1%. The increase in rate of an MCE per Gy MHD for a patient with at least 1 cardiac risk factor is 19.6% in the first 4 years after exposure, and death rate from MCE per Gy MHD increases 13.6% in the first 4 years. Compared with 3-D conformal planning, VMAT reduced the MHD by as much as 7 Gy in this case. Therefore, the risk of having an MCE after RT for this patient was reduced with VMAT by as high as 137.2% compared to the 3D conformal plans, and the risk of death from ischemic heart disease (IHD) was reduced by as much as 95.2%.
A recent study investigated short-term pulmonary radiation pneumonitis (RP) using changes in pulmonary function tests (PFTs) after locoregional radiation therapy (LRRT)13 in which regional nodal irradiation (RNI) included the IMNs. The constraint for the ipsilateral lung V20 Gy was < 30%. Chemotherapy included cyclophosphamide and taxanes and was concluded 3-4 weeks before initiating RT. By adhering to this constraint, incidence of symptomatic RP was ~6% (both grade 1 and 2) and no grade 3 or 4 pneumonitis was observed. In an earlier study by the same group, 475 patients with breast cancer who had received RT were followed for pulmonary complications at 1, 4 and 7 months post treatment.14 Patients who received locoregional RT that included the IMNs while maintaining the ipsilateral lung V20 Gy around 30%, showed 5.5% grade 1 and 11% grade 2 complication rates. Patients for whom the V20 Gy was around 35% showed a 23% grade 1 and 11.5% grade 2 complication rate. Goldman et al13 concluded that by reducing the V20 Gy to < 30% they could reduce the rates of short-term RP and changes in short-term pulmonary function compared to patients in the earlier study by Lind et al.14 Varga et al21 have shown that use of sequential taxane-based chemotherapy in treating patients for chest wall and regional nodes including IMNs with adjuvant RT showed no incidence of RP or lung fibrosis. In these patients, the V20 Gy on average was 29% ± 1.1%.21 The risk of acute and chronic RT-induced lung morbidity is influenced by the irradiated lung volume, total dose and dose per fraction.22,23 In this case, we could maintain the ipsilateral lung V20 Gy < 30% with VMAT, but not with 3-dimensional conformal radiation therapy (3DCRT).
VMAT, however, increased the volume of the heart and the lung covered with low dose. For this case, the heart V5 Gy was 37% with PWT, 48% with VMAT and 78% with photon/electron mix technique. The influence of low dose—specifically the volume of the heart covered by 1 to 2 Gy with RT on heart disease—has been investigated in the literature.24 No correlation was found between low dose and cardiac perfusion defects or function, and there was no worsening of these defects within a short-term follow-up (1 year) after exposure. However, the MHD for all patients in the Chung study was < 6.1 Gy (6.4 Gy in this case study). Hence, even though PWT best spared the volume of the heart covered with low dose, the MHD was more than double that with VMAT due to increased volume of the heart covered by higher doses with MHD. The study cautioned that a dose-response relationship in the short term might exist at higher doses. A combination of VMAT and deep inspiration breath hold (DIBH) can provide a cumulative benefit in further minimizing heart exposure for patients treated with locoregional RT of left-sided breast cancer.25 Compared with VMAT alone, a combination of VMAT and DIBH can reduce the MHD on average by 2.9 Gy (1.5 Gy – 4.3 Gy).26 The volume of the lungs receiving low dose is also increased with VMAT compared to standard 3D conformal techniques. However, no grade 3 or higher pneumonitis rates have been observed, even when the ipsilateral lung V5 Gy was 100%.27 Moreover, incidence of secondary cancers after RT has a latency of onset ≥ 10 years after initial treatment,28 and is unlikely to manifest in this case.
FOLLOW-UP
The patient developed progressive hyperpigmentation and erythema of the irradiated left chest wall, and dry desquamation was noted at a dose of 3420 cGy. On Sept. 2, 2014, the patient successfully completed RT as planned, and during the last week of treatment she developed patchy areas of moist desquamation (NCI CTCAE v4.0 Grade 2-3), most pronounced in the region of the mastectomy scar. The skin reaction was managed with topical emollients and petrolatum gauze dressings. Discomfort was managed effectively with over-the-counter analgesics, and she completed treatment without interruption.
At follow-up 2 months later (delayed due to interval surgery for prophylactic bilateral salpingo-oophorectomy), she reported feeling well overall. She denied any specific chest wall complaints other than a sensation of tightness in the left upper extremity and lateral chest wall. Physical examination was notable for mild residual hyperpigmentation of the left chest wall with no overt desquamation. The left chest wall skin and subcutaneous tissue appeared mildly thickened and indurated but without discrete palpable lesions. There was no upper extremity lymphedema. She was referred to physical therapy for management of the upper extremity symptoms, which improved with range of motion exercises. No evidence of lymphedema was noted in follow-up visits at 9, 12 and 15 months post treatment. At 9 months post treatment, she was diagnosed with metastatic disease (brain, bone and contralateral internal mammary nodes), and was treated with further chemotherapy and palliative irradiation of brain and osseous metastases. She returned for follow up in April 2016 and had no symptoms suggesting cardiovascular or respiratory compromise. No evidence of chest wall or ipsilateral regional nodal recurrence was present.
CONCLUSION
We present a case of a patient diagnosed with IBC of the TN subtype, which is an aggressive disease. Multimodality treatment included chemotherapy, surgery and radiation. The need to cover the chest wall and regional nodes combined with unfavorable anatomy required the use of advanced RT planning and delivery techniques other than standard 3D conformal methods. In this case, VMAT was able to best spare the heart and the lung without sacrificing target coverage, outweighing the risk of secondary cancer.
REFERENCES
- Li J, Gonzalez-Angulo AM, Allen PK, et al. Triple-negative subtype predicts poor overall survival and high locoregional relapse in inflammatory breast cancer. Oncologist. 2011;16:1675-1683.
- Saigal K, Hurley J, Takita C, et al. Risk factors for locoregional failure in patients with inflammatory breast cancer treated with trimodality therapy. Clin Breast Cancer. 2013;13(5):335-343.
- Liao Z, Strom EA, Buzdar AU, et al. Locoregional irradiation for inflammatory breast cancer: effectiveness of dose escalation in decreasing recurrence. Int J Radiat Oncol Biol Phys. 2000;47:1191-1200.
- Bristol IJ, Woodward WA, Strom EA, et al. Locoregional treatment outcomes after multimodality management of imflammatory breast cancer. Int J Radiat Oncol Biol Phys. 2008;72:474-484.
- Damast S, Ho AY, Montgomery L, et al. Locoregional outcomes of inflammatory breast cancer patients treated with standard fractionation radiation and daily skin bolus in the taxane era. Int J Radiat Oncol Biol Phys. 2010;77:1105-1112.
- Lehne G, Lote K. Pulmonary toxicity of cytotoxic and immunosuppressive agents. A review. Acta Oncol. 1990;29(2):113-124.
- Beal K, Hudis C, Norton L, et al. Radiation pneumonitis in breast cancer pateints treated with taxanes: Does sequential radiation therapy lower the risk? Breast J. 2005;11(5):317-320.
- Pierce LJ, Butler JB, Martel MK, et al. Postmastectomy radiotherapy of the chest wall: Dosimetric comparison of common techniques. Int J Radiat Oncol Biol Phys. 2002;52(5):1220-1230.
- Marks LB, Hebert ME, Bentel G, et al. To treat or not to treat the internal mammary nodes: a possible compromise. Int J Radiat Oncol Biol Phys. 1994;29(4):903-909.
- Dumane VA, Hunt MA, Green S, et al. Dosimetric comparison of volumetric modulated arc therapy, static field intensity modulated radiation therapy, and 3D conformal planning for treatment of a right-sided reconstructed chest wall and regional nodal case. J Radiother. 2014;1-12.
- Klein EE, Marie Taylor MS, Michaletz-Lorenz M, et al. A mono isocentric technique for breast and regional nodal therapy using dual asymmetric jaws. Int J Radiat Oncol Biol Phys. 1994;28(3):753-760.
- Darby SC, Ewertz M, McGale P, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987-998.
- Goldman UB, Anderson M, Wennberg B, et al. Radiation pneumonitis and pulmonary function with lung dose-volume constraints in breast cancer irradiation. J Radiother Pract. 2014;13:211-217.
- Lind, B. Wennberg, G. Gagliardi et al. Pulmonary complications following different radiotherapy techniques for breast cancer, and the association to irradiated lung volume and dose. Breast Cancer Res Treat. 2001;68:199-210.
- Kong FM, Klein EE, Bradley JD, et al. The impact of central lung distance, maximal heart distance, and radiation technique on the volumetric dose of the lung and heart for intact breast radiation. Int J Radiat Oncol Biol Phys. 2002;54(3):963-971.
- Popescu CC, Olivotto I, Patenaude V, et al. Inverse planned, dynamic, multi-beam, intensity-modulated radiation therapy (IMRT): a promising technique when target volume is the left breast and internal mammary lymph nodes. Med Dosim. 2006;31(4):283-291.
- Beckham WA, Popescu CC, Patenaude VV, et al. Is multibeam IMRT better than standard treatment for patients with left-sided breast cancer? Int J Radiat Oncol Biol Phys. 2007;69(3):918-924.
- Popescu CC, Olivotto IA, Beckham WA, et al. Volumetric modulated arc therapy improves dosimetry and reduces treatment time compared to conventional intensity-modulated radiotherapy for locoregional radiotherapy of left-sided breast cancer and internal mammary nodes. Int J Radiat Oncol Biol Phys. 2010;76(1):287-295.
- Dumane VA, Lazarev S, Sheu R, et al. Optimizing treatment positioning to achieve better heart sparing in a left-sided, whole-breast irradiation case unfit for deep-inspiration breath-hold treatment. Appl Radiat Oncol. 2016;28-32.
- Radiation Therapy Oncology Group. RTOG Breast Cancer Contouring Atlas. https://www.rtog.org/CoreLab/ContouringAtlases/BreastCancerAtlas.aspx. Accessed July 16, 2014.
- Varga Z, Cserhati A, Kelemen G, et al. Role of systemic therapy in the development of lung sequelae after conformal radiotherapy in breast cancer patients. Int J Radiat Oncol Biol Phys. 2011;80(4):1109-1116.
- Overgaard M, Bentzen SM, Christensen JJ, et al. The value of the NSD formula in equation of acute and late radiation complications in normal tissue following 2 and 5 fractions per week in breast cancer patients treated with postmastectomy irradiation. Radiother Oncol. 1987;9(1):1-11.
- Rothwell RI, Kelly SA, Joslin CA. Radiation pneumonitis in patients treated for breast cancer. Radiother Oncol. 1985;4(1):9-14.
- Chung E, Corbett JR, Moran JM, et al. Is there a dose-response relationship for heart disease with low-dose radiation therapy? Int J Radiat Oncol Biol Phys. 2013;85(4):959-964.
- Osman SOS, Hol S, Poortmans PM, et al. Volumetric modulated arc therapy and breath-hold in image-guided locoregional left-sided breast irradiation. Radiother Oncol. 2014;112:17-22.
- Dumane VA, Saksornchai K, Zhou y, et al. Quantifying the effects of combining deep inspiration breath hold (DIBH) with volumetric modulated arc therapy (VMAT) in breast cancer patients receiving regional nodal irradiation (RNI). Int J Radiat Oncol Biol Phys. 2016;96(2S):E681.
- Ho AY, Ballangrud AM, Li G, et al. Pneumonitis rates following comprehensive nodal irradiation in breast cancer patients: results of a phase I feasibility trial of intensity modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2013;87(2): S48-S49.
- Ng J, Shuryak I. Minimizing second cancer risk following radiotherapy: current perspectives. Cancer Manag Res. 2015;7:1-11.
Citation
VA D, N O, S G. Volumetric-modulated arc therapy improved heart and lung sparing for a left-sided chest wall and regional nodal irradiation case. Appl Radiat Oncol. 2017;(3):28-36.
September 21, 2017