Stereotactic Body Radiation Therapy for Oligometastatic Spine Disease
Images
Oligometastatic disease (OMD) is an intermediate stage of cancer between an isolated tumor and widespread metastatic disease, where cancer cells from the primary tumor travel through the body/bloodstream to form a small number of clinically detectable metastatic lesions – typically less than 5 – elsewhere in the body. It is a disease state in which therapy may enable long-term disease management, much like with diabetes and heart disease, and unlike prior paradigms where metastatic disease was incurable, treatment may be potentially curative.1
From Fatal to Chronic
“Our overall goal is to make stage 4 cancer well-controlled, so it becomes more of a chronic illness than a deadly disease,” says Yoshiya (Josh) Yamada, MD, co-chief of Multidisciplinary Spine Tumor Service at Memorial Sloan Kettering Cancer Center (MSKCC). “In oligometastatic disease, stage 4 is very controllable with a good prognosis for patients. Many of us in oncology are very excited to see this vision we had 5 years ago now becoming a reality.”
OMD is believed to be a precursor to more aggressive stage 4 disease, says Dr. Yamada, and stereotactic body radiation therapy (SBRT) is a cornerstone for treating oligometastatic patients. “If you believe the oligometastatic disease paradigm, then early intervention should make a difference,” she says.
Kristin Janson Redmond, MD, MPH, an associate professor of Radiation Oncology and Molecular Radiation Sciences at Johns Hopkins Medicine who leads the institution’s spinal radiosurgery program, frequently uses SBRT for spine oligometastases. “We hypothesize that SBRT may provide a unique opportunity for durable, long-term local control in patients with oligometastases,” says Dr. Redmond. “If we truly control those few sites, we may be able to prevent other metastases from arising and, thereby, actually improve their overall survival compared to patients with widely metastatic disease where the goal of local therapy is palliation.”
The perception is that if cancer spread is minimal, the patient may live longer and potentially be cured, says Mitchell C. C. Liu, MDCM, FRCPC, clinical associate professor at the University of British Columbia, Disease Site Leader of Lung Cancer, and a leader in SBRT in radiation oncology at the British Columbia Cancer, Vancouver Center. “This can be difficult for some oncologists to accept, as most of us learned in medical school that cancer is incurable once it has spread. So, oligometastatic disease is changing what we were taught.”
Patient Selection
Careful patient selection and the ability to provide local control and durable pain relief for patients with spine metastases are crucial elements to optimizing treatment. For patients to benefit from SBRT for spine oligometastases, they should have presumed better survival as well as good prognostic features, specifically young age, patient fitness, slow-growing cancers, and minimal disease burden.2
“Specifically for spine SBRT, radioresistant pathology such as renal cell, melanoma, sarcoma and colorectal seem to benefit better with higher dose per fraction, with SBRT likely to give a more durable local control compared to conventional palliative radiotherapy,” he says.
Some patients may also need surgery before SBRT for spine OMD, notes Dr. Redmond. “If a patient has a lot of epidural disease, we will need to underdose the gross disease adjacent to the spinal cord in order to keep the treatment plan safe. These patients may benefit from surgery (first) to downgrade their epidural disease and optimize their outcome.”
Local and Systemic Treatment
The use of systemic therapy is patient- and disease-specific. One approach is to use SBRT for local control and then employ systemic therapies if the patient develops disease in other sites.
If a patient is truly oligometastatic, that individual will not likely need systemic therapy after irradiating the known disease, adds Dr. Liu. However, identifying all metastatic disease in a patient can prove challenging. “We don’t have a way of knowing if [OMD is present] because our technology limits how well we can detect all the metastatic lesions or cells in a patient’s body,” he says. Emerging technologies may help, such as circulating tumor DNA, which is a biomarker of a biological molecule found in the bloodstream that flags disease.
Another approach is to use certain systemic agents to help improve local control of the SBRT treatment or use SBRT to improve effectiveness of systemic therapy. “SBRT may enhance immunogenicity of a tumor, making it more likely that the immune system can attack it,” says Dr. Yamada.
Dose and Fractionation
There is no broad consensus on the optimal dose fractionation when using SBRT for spine oligometastases. Dr. Liu believes it will be extremely difficult to determine the ideal treatment regimen without a large phase 3 study. Consequently, each institution must prescribe the best treatment for individual patients that aligns with the institution’s or oncologist’s experience and comfort level.
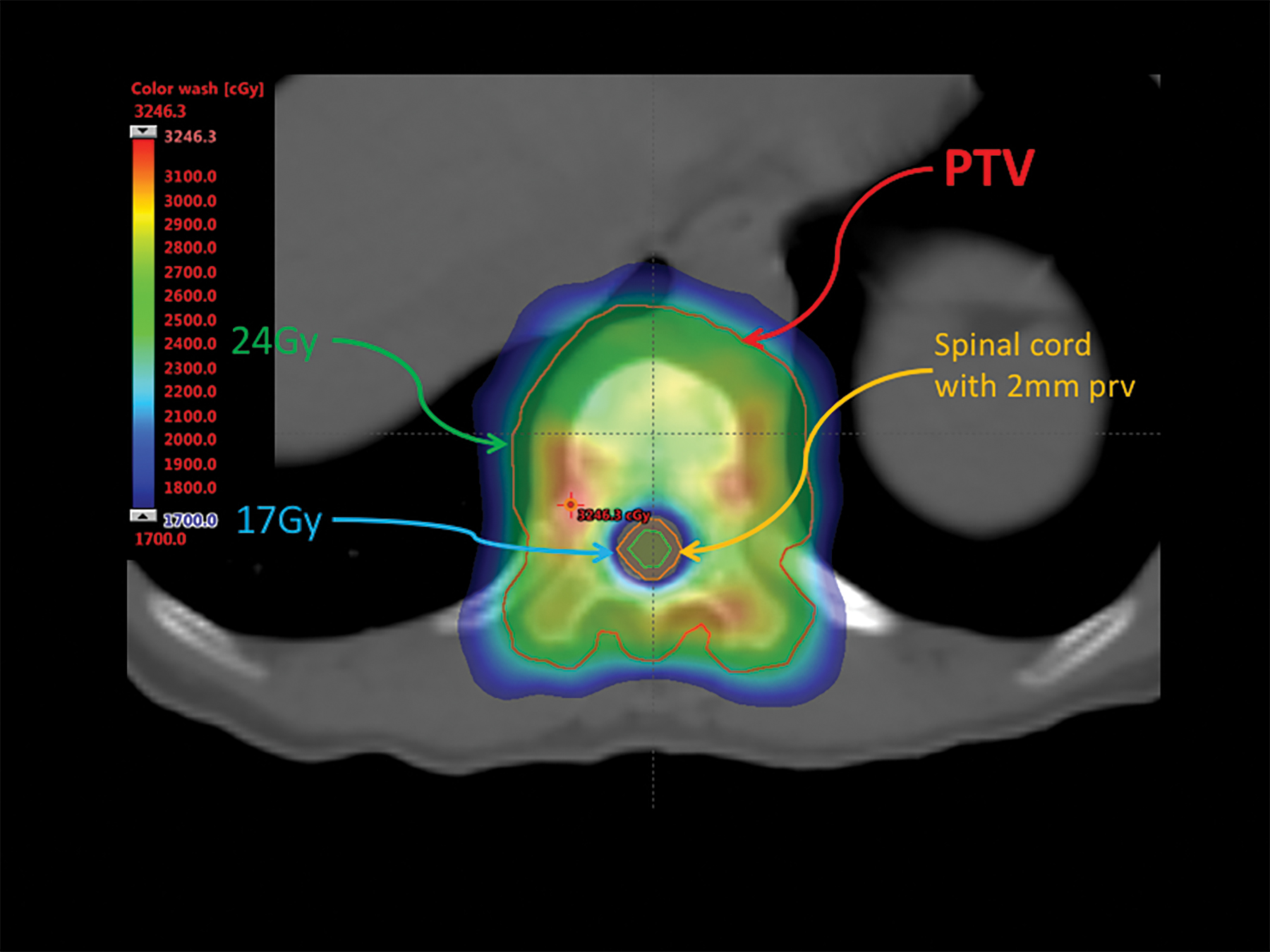
“Ten years ago, we started with 35 Gy and 5 fractions because we were not that experienced with SBRT and we perceived that more fraction numbers appeared to be safer,” Dr. Liu explains. “Now we are moving to 24 Gy/2 fractions and some of our oncologists are more comfortable with this prescription.” (Figure 1)
Dr. Liu says in the range of 20 Gy/1 is also appropriate; however, preliminary results from RTOG 0631 showed that 16 Gy/1 did not improve pain control compared with conventional palliative radiation. Thus, a higher dose than 16 Gy is likely necessary,3 he says. Final results on whether 16 Gy may provide better local control are eagerly awaited.
Dr. Redmond typically uses 24 Gy/2 in her practice. If she cannot meet the core constraints in 2 fractions, she uses 27 Gy/3. Control rates with SBRT for spine metastases in her practice are around 90 percent, she notes, adding that data comparing outcomes using different prescription doses is lacking, and interpreting existing data is complex. For example, a treatment plan prescribing to the 50 or 60 percent isodose line would be substantially “hotter” than the same prescription delivered to the 80 or 90 percent isodose line.
“The reason I use 2 fractions is the increasing body of literature of the risk of fracture in the spine induced by the radiation,” Dr. Redmond says. “By reducing the dose per fraction, we believe we can decrease that fracture risk, although it is highly variable across practices.”
That “ground truth” of whether more fractionated regimens are as effective as single-fraction treatments is unknown without a head-to-head study, she adds.
At MSKCC, Dr. Yamada uses 24 Gy/1 in his practice. “We are a little more aggressive than other centers. Our experience and data suggest that the highest dose level – 24 Gy, 1 fraction – is really an ablative dose with local failure around 2.3 percent at 4 years.”
In a study by Tseng et al, the use of 24 Gy/2 resulted in a cumulative local failure rate of 17 percent.4 Yet, higher single doses are not for everyone, he says. A single high dose may be unsafe in patients with large tumors, where the risk of exposing the esophagus is high. If the tumor is in the spinal canal, a high dose may enter the spinal cord, leading to additional complications. Patients who were previously irradiated are also not offered 24 Gy/1 at MSKCC, although Dr. Yamada says the institution is actively recruiting patients to further study this protocol.
Patient Response
The biggest predictor of survival for patients with spine oligometastases is whether the disease is truly oligometastatic. “Overall survival is dictated by the big picture,” says Dr. Redmond. “Sometimes a few months after treatment the patient will develop other sites of disease. It also depends on the systemic options that patients have and whether or not they can be salvaged if more sites of the disease arise.”
More high-quality randomized trials are needed to compare different treatments, prescriptions, and techniques, she adds, to help oncologists optimize local control and minimize toxicity.
Some metastatic pathologies, such as breast, prostate and renal cancers, have been shown to have favorable outcomes when treated with SBRT,5 Dr. Liu says. He also cites a recent study by Milano et al that reported women with breast-bone-only oligometastases treated with SBRT had an 83 percent overall survival rate at 5 years and a 75 percent survival rate at 10 years. All 12 patients with bone-only oligometastases treated had no local recurrence at 2-, 5- and 10-year follow-up, and 67 percent had no widespread metastases at 5- and 10-year follow-up.6
Dr. Liu hopes the results of the Canadian Cancer Trials Group SC247 comparing 24 Gy/2 vs palliative radiation therapy will be presented soon. He would also like to see more investigation on the use of systemic therapy, including the best time to deliver it in conjunction with spine SBRT.
“Is it better to use systemic therapies before SBRT and, if so, when is the best timing for SBRT? Is it for persistent residual disease or at the first sign of recurrence?” Dr. Liu poses. “In the setting where surgery is required, what is the role of preoperative SBRT instead of the more conventional post-op SBRT, where it can be more challenging to contour the targets and organs at risk due to artifacts. And, if pre-op SBRT is doable, what is the optimal dose and timing?”
Dr. Yamada says the safest way to re-irradiate with high doses that provide durable tumor control is with SBRT. “SBRT is a biologically different treatment,” she states. “In our data, patients who received salvage SBRT after prior radiation treatment on tumors that required surgical intervention had outcomes just as good as the patients who never had radiation before SBRT. I think SBRT is really becoming a preferred treatment approach for patients who have been previously irradiated, and that is especially true for all metastatic patients.”
Team Approach
A key component in treating spine metastases is multidisciplinary care, Dr. Yamada adds. A team of radiation oncologists, orthopedic surgeons, neurosurgeons, physiatrists, radiologists and interventionalists all work together at MSKCC to develop a comprehensive plan that individualizes each patient’s treatment plan.
“It is absolutely a key component of our program that we are able to function in a multidisciplinary environment,” she stresses. “I think without that, SBRT probably would not have flourished at our institution, and I imagine that’s the same in many other centers.”
Yet, SBRT may not be an option for all patients, Dr. Redmond cautions. “Ultimately, when looking at the patient’s best interest, if they don’t have access to high-quality SBRT, they are actually better off having conventional radiation that is done well,” she says. “If you are doing a very precise therapy like SBRT incorrectly, you could miss the target or overdose the spinal cord.”
References
- Nowee M. Oligometastases: improving outcomes for a newly identified stage of cancer. Oncol Times. 2020;42(2):1,8,13. doi:10.1097/01.COT.0000653236.29169.ff
- Palma DA, Louie AV, Rodrigues GB. New strategies in stereotactic radiotherapy for oligometastases. Clin Cancer Res. 2015;21(23):5198-5204. doi:10.1158/1078-0432.CCR-15-0822
- Ryu S, Pugh SL, Gerszten PC, et al. RTOG 0631 phase 2/3 study of image guided stereotactic radiosurgery for localized (1-3) spine metastases: phase 2 results. Pract Radiat Oncol. 2014;4(2):76-81. doi:10.1016/j.prro.2013.05.001
- Tseng CL, Soliman H, Myrehaug S, et al. Imaging-based outcomes for 24 gy in 2 daily fractions for patients with de novo spinal metastases treated with spine stereotactic body radiation therapy (SBRT). Int J Radiat Oncol Biol Phys. 2018;102(3):499-507. doi:10.1016/j.ijrobp.2018.06.047
- Hong JC, Ayala-Peacock DN, Lee J, et al. Classification for long-term survival in oligometastatic patients treated with ablative radiotherapy: a multi-institutional pooled analysis. PLoS One. 2018;13(4):e0195149. doi:10.1371/journal.pone.0195149
- Milano MT, Katz AW, Zhang H, Huggins CF, Aujla KS, Okunieff P. Oligometastatic breast cancer treated with hypofractionated stereotactic radiotherapy: some patients survive longer than a decade. Radiother Oncol. 2019;131:45-51 doi:10.1016/j.radonc.2018.11.022
- NIH U.S. National Library of Medicine. Clinical Trials.gov. Study comparing stereotactic body radiotherapy vs conventional palliative radiotherapy (CRT) for spinal metastases. ClinicalTrials.gov Identifier: NCT02512965. Accessed August 13, 2020. https://clinicaltrials.gov/ct2/show/NCT02512965
Citation
MB M. Stereotactic Body Radiation Therapy for Oligometastatic Spine Disease. Appl Radiat Oncol. 2020;(3):30-31.
September 9, 2020