Radiation Recall Dermatitis with Docetaxel and Cyclophosphamide in a Case of Early Stage Breast Cancer Considered High Risk
Images


CASE SUMMARY
The patient was a 55-year-old woman with an unremarkable history, presenting with a screen-detected mass on the left breast. Biopsy revealed grade II invasive ductal carcinoma, ER/PR-positive, HER2/neu-negative, and a Ki-67 of 5%.
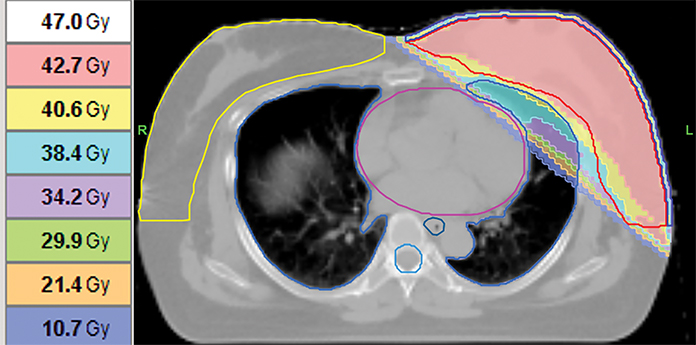
Lumpectomy and sentinel lymph node biopsy yielded a 0.5 cm tumor and 2 uninvolved lymph nodes. Chemotherapy was not considered outright due to perceived low-risk clinical features; specimens were instead sent out for gene profiling to guide systemic therapy. Whole-breast radiation therapy to 42.6 Gy (16 fractions) was initiated 4 weeks after surgery (Figure 1). Only grade 1 radiation dermatitis (NCI-CTCAE v. 4.03)1 was observed.
Results from gene profiling (MammaPrint, Agendia, Inc.) arrived later, revealing high-risk luminal B disease, indicating a benefit from chemotherapy. Docetaxel (75 mg/m2) and cyclophosphamide (600 mg/m2) were given 4 weeks after completing radiation therapy. On the second day of chemotherapy, the patient developed linear, erythematous, pruritic, nonpainful plaques on the left breast, corresponding to the previously irradiated area (Figure 2).
DIAGNOSIS AND TREATMENT
The reaction, atypical of a chemotherapeutic side effect, was ascribed to radiation recall dermatitis. The symptoms were managed with oral cetirizine and betamethasone cream and it subsided to dry desquamation within 2 weeks (Figure 3).
Pulsed steroids were given with subsequent cycles of chemotherapy using the same agents and no recurrences of the reaction were observed. The patient completed 4 cycles of treatment.
DISCUSSION
Radiation recall dermatitis (RRD) is an acute inflammatory reaction occurring in previously irradiated sites, triggered by a variety of chemotherapeutic agents, including conventional medications such as anthrayclines, taxanes, and antimetabolites.2-4 More contemporary agents5 have also elicited this reaction.
A review by Burris and Hurtig documented RRD involving other drug classes.2 Notably, several of the implicated agents are drugs commonly used in the treatment of breast cancer.1,5
Data regarding the frequency of this phenomenon has been limited and most information has been documented through case reports. Rates from 1.8% to 15.1% have been reported.2 In an observational study by Kodym et al, 8.8% of 91 patients who received sequential palliative radiation therapy and chemotherapy developed a reaction.6
D’Angio first described RRD with actinomycin in 19597 but the heterogeneity of the cases reported has precluded a definitive characterization of the reaction and it remains a poorly understood phenomenon. Its occurrence is difficult to predict with incidences occurring months to years after radiation therapy. The drugs implicated differ from one person to another. The pathophysiology is also unclear, with several theories describing vascular damage, stem cell inadequacy, epithelial stem cell sensitivity, and drug hypersensitivity as possible etiologies. There is no clear threshold dose and it can develop at doses from 10 Gy to 61.2 Gy.1,8
Although RRD can occur over a wide range of time intervals between treatments, some evidence points to a shorter duration as a risk factor. In the American Society of Breast Surgeons Mammosite breast brachytherapy trial, accelerated partial breast irradiation (APBI) was given prior to chemotherapy. Adjuvant doxorubicin was given to 75% of patients and RRD was identified in 15 out of 131 (11.4%) patients. The time interval between completion of brachytherapy to the start of chemotherapy was a significant factor to its development, with an 18% occurrence in those who received chemotherapy < 3 weeks after APBI in contrast to 7.4% for an interval > 3 weeks (p = 0.09).9
A more complex interplay between total dose and time interval may exist, as shown by the development of RRD in a field treated to 38 Gy 7 days prior to etoposide administration but not in another site treated to 45 Gy 8 months before. The severity of the skin reaction during radiation therapy has not been correlated with the risk of developing RRD.8
The route of administration also affects the natural history of RRD. Agents given intravenously elicit the reaction rapidly while oral agents are protracted in development. The resolution of lesions seems to follow a similar pattern: Reactions from intravenous drugs have been observed to disappear more promptly than reactions from oral drugs.2
RRD may be approached in several ways and most cases are managed symptomatically. Observation is sufficient if there is only a mild, tolerable reaction. Steroids, NSAIDS, and anti-histamines can be used to reduce inflammation. In severe cases, the implicated drugs should be withheld as lesions rarely heal with continuation of medications.
A drug re-challenge is a viable option. Among factors to consider are patient-physician preference and the extent of RRD. Some may choose to lower the dose while others attempt premedication to prevent the inflammatory response. Alternative chemotherapy regimens may also be explored.2,8
The high prevalence of breast cancer combined with changing treatment paradigms predicts for a potential increased risk of RRD. Most of our information comes from well-described case reports and series; however, the rarity of the condition, the inability to predict which patient groups develop the reaction, the lack of a database, and the heterogeneity among cases have precluded a definitive characterization of this risk.
We have demonstrated that symptom control, re-challenge with the RRD-triggering drug, and premedication can be employed successfully. In this situation, we highlight the increasing use of molecular profiling to guide chemotherapy utilization in patients who otherwise have a clinically low risk of recurrence. Chemotherapy might not be part of initial management plans due to the time-lag from the arrival of results. The usual sequence of giving radiation therapy after chemotherapy is reversed and this potentially increases the risk of RRD.
CONCLUSION
Although current figures indicate that RRD is rare, the symptoms are easily identifiable and the reaction can be effectively controlled. Risk factors have been identified but these are not uniform across all patients with RRD. One of the most critical elements we need is how to identify those at greatest risk of developing it. A database may be useful to characterize this reaction. This crucial body of data can help clinicians predict, identify, and treat RRD, especially in the setting of increased utilization of adjuvant treatment.
REFERENCES
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) version 4.03: June 14, 2010.
- Burris HA, Hurtig J. Radiation recall with anticancer agents. Oncologist. 2010;15(11):1227-1237.
- Hird AE, Wilson J, Symons S, Sinclair E, Davis M, Chow E. Radiation recall dermatitis: case report and review of the literature. Curr Oncol. 2008;15(1).
- Azria D, Magne N, Zouhair A, et al. Radiation recall: a well recognized but neglected phenomenon. Cancer Treat Rev. 2005;31(7):555-570.
- Levy A, Hollebecque A, Bourgier C et al. Targeted therapy-induced radiation recall. Eur J Cancer. 2013;49(7):1662-1668.
- Kodym E, Kalinska R, Ehringfeld C, Sterbik-Lamina A, Kodym R, Hohenberg G. Frequency of radiation recall dermatitis in adult cancer patients. Oncol Res Treat. 2004;28(1):18-21.
- D’Angio GJ, Sidney F, Maddock CL. Potentiation of X-Ray effects by Actinomycin D. Radiology. 1959;73(2):175-177.
- Camidge R, Price A. Characterizing the phenomenon of radiation recall dermatitis. Radiother Oncol. 2001(59)3:237-245.
- Haffty BG, Vicini FA, Beitsch P, et al. Timing of chemotherapy after MammoSite radiation therapy system breast brachytherapy: analysis of the American Society of Breast Surgeons MammoSite breast brachytherapy registry trial. Int J Rad Oncol Biol Phys. 2008;72(5):1441-1448.
Citation
JPF A, KH B. Radiation Recall Dermatitis with Docetaxel and Cyclophosphamide in a Case of Early Stage Breast Cancer Considered High Risk. Appl Radiat Oncol. 2020;(3):46-48.
September 9, 2020