Controversies in the preoperative radiotherapeutic management of resectable esophageal cancer
Images
SA-CME credits are available for this article here.
Esophageal cancer remains the 7th leading cause of cancer death in the United States with annual incidence and mortality of 17,290 and 15,580 individuals, respectively.1 Several strategies have been employed over the years to improve outcomes. Initial studies comparing surgery to radiation therapy (RT) showed high operative mortality in surgical patients, and poor survival in both the surgical and radiation-alone patients.2 In the 1990s, improvements in survival were made with the addition of concurrent chemotherapy to RT,3,4 with no patients alive at 3 years in the RT-alone arm. The 2- and 5-year overall survival rates in definitive chemoradiation (CRT) were 35% to 40%, and 20%, respectively, with local failure rates of 45% to 55%.5-7 To improve these outcomes, the use of surgical resection after chemoradiation was investigated.8-13
In this review, we examine the role of trimodality therapy in the management of locally advanced esophageal cancer, focusing on controversies surrounding the optimal total neoadjuvant RT dose employed. We will additionally review the current and past technologies for radiation treatment delivery, and their impact on overall survival and toxicity in this patient cohort.
A Review of Prior Phase III Concurrent Chemoradiation Trials
Studies Comparing Neoadjuvant CRT Followed by Surgery to Definitive CRT
Two randomized trials have compared the use of definitive CRT to neoadjuvant CRT followed by surgical resection. The German Esophageal Study Group performed a phase III trial comparing definitive CRT to preoperative CRT followed by resection in locally advanced squamous cell carcinoma of the esophagus. Patients were randomized to induction chemotherapy (5-FU, leucovorin, etoposide and cisplatin) followed by CRT (40 Gy) and surgical resection or induction chemotherapy (5-FU, leucovorin, etoposide and cisplatin) followed by CRT (at least 65 Gy) without surgical resection.5 At a median follow-up of 6 years, overall survival was equivalent between the arms, with improvements in local progression-free survival in the surgery group (p = 0.003), but at the cost of a 9% higher risk of treatment-related mortality (p = 0.03). The FFCD 9102 trial randomized 444 patients with resectable esophageal cancer (majority squamous histology) to induction CRT consisting of either 46 Gy in 23 fractions with concurrent cisplatin and 5-FU or split course 30 Gy in 10 fractions RT given over 4 weeks (5 days on, 10 days off, 5 days on).7 Responders proceeded to surgical resection while nonresponders completed chemoradiation to a total dose of either 66 Gy in 33 fractions (standard fractionation) or 45 Gy in 15 fractions (for the hypofractionated arm). At 4 years median follow-up, there was no difference in overall survival between the groups (2-year OS of 39.8% vs. 33.6%, p = 0.03). However, improved local control was observed in the surgery arm at 66.4% compared with 57.0% in the definitive CRT arm, but with higher acute, 3-month mortality in the surgical group (9.3% vs. 0.8%).
A meta-analysis of 7 studies and 1,114 patients compared surgical with nonsurgical management of esophageal cancer.14 When comparing definitive CRT to neoadjuvant CRT followed by surgery, there was no difference in long-term recurrence or mortality (HR = 0.88). The impact of cancer histology could not be adequately assessed since most trials were limited to squamous cell carcinoma (SCC) only. The evidence in these studies was considered low or very low based on trial size and design and, therefore, strong conclusions cannot be derived from this data. Future work is needed in this arena.
Studies Comparing Neoadjuvant CRT Followed by Surgery to Surgery Alone
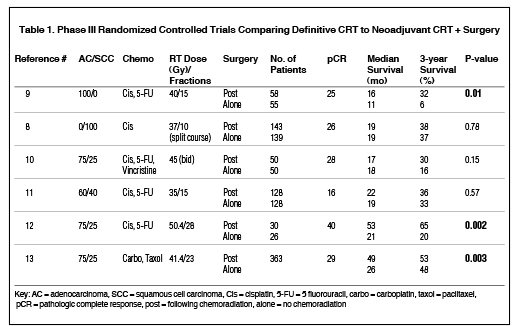
Multiple studies have evaluated the outcomes of neoadjuvant chemoradiation followed by surgical resection with surgical resection alone (Table 1).8-13 Walsh et al evaluated outcomes of esophageal adenocarcinoma (AC) patients treated with 40 Gy in 15 fractions of RT combined with cisplatin and 5-fluorouracil (5-FU) chemotherapy followed by surgical resection compared with surgical resection alone. Three-year survival improved from 6% in the surgery alone arm to 32% in the trimodality arm (p = 0.01), and pathologic complete response (pCR) at time of surgical resection was 25%.9 Similarly, the European Organization for Research and Treatment of Cancer (EORTC) trial8 randomized SCC patients to surgery alone or neoadjuvant CRT consisting of two 1-week courses of RT, separated by a 2-week break, to a total dose of 37 Gy in 10 fractions with concurrent cisplatin. A pCR rate of 26% was noted, with equivalent 3-year overall survival near 36%. Urba et al compared concurrent cisplatin, 5-FU and vincristine with 45 Gy radiation given twice-daily (BID) to surgery alone in a study population of 100 patients with mostly AC histology (3:1 AC to SCC ratio in both arms). Trial results demonstrated a pCR rate of 28% and a numerical, but not statistically significant, improvement in survival (3-year OS of 30 months vs. 16 months in the neoadjuvant CRT vs. surgery arms, p = 0.15). The Trans Tasman Radiation Oncology Group (TROG) randomized trial compared cisplatin, 5-FU and 35 Gy in 15 fractions followed by surgical resection with surgical resection alone in a study population of SCC and AC patients. No survival difference was observed (3-year survival of 36 months vs. 33 months in neoadjuvant CRT vs. surgery, p = 0.57), with pCR rates of 16%.11
In the Cancer and Leukemia Group B (CALGB) trial, 56 patients were randomized to either surgery alone or surgery following neoadjuvant CRT with 50.4 Gy in 28 fractions plus cisplatin and 5-FU.12 The trial showed a significant improvement in overall survival (5-year OS of 39% vs. 16%, p = 0.002). The ChemoRadiotherapy for Oesophageal Cancer Followed by Surgery Study (CROSS) trial randomized 368 patients with resectable esophageal cancer (75% AC) to a new better tolerated CRT regimen of carboplatin and paclitaxel combined with 41.4 Gy in 23 fractions followed by surgical resection to surgical resection alone.13 These impressive results included a 5-year OS of 47% vs. 34% in the neoadjuvant CRT vs. surgery alone arms (p = 0.003). Neoadjuvant treatment resulted in an overall pCR rate of 29% (49% for SCC, 23% for AC, p = 0.008), and an increased rate of R0 resection (92% vs. 69%, p < 0.001). These improvements were achieved without an increase in acute complication rates, which remained below 5% in both study arms.
Finally, a meta-analysis of trials from 2007 suggested a 13% absolute difference in survival at 2 years (HR 0.81) with the addition of neoadjuvant CRT to surgery, thus confirming the benefit of preoperative CRT.15
Controversies in Radiation Dose and Planning Considerations for Preoperative Resectable Esophageal Cancer
The studies shown in Table 1 vary widely with total dose and fractionation schemes ranging from daily 2 Gy fractions to hypofractionated split courses of radiation with 2-week breaks to BID regimens. Total doses of radiation have ranged from 30 Gy to as high as 50.4 Gy in patients who were eligible to undergo surgical resection. The debate of dose-escalation has been tested in a randomized clinical trial6 in the setting of definitive chemoradiation, and the question remains unanswered at this point in time. Although improved local control is noted in higher dose fractionations,6,16,17 translation into an overall survival benefit remains to be seen in this population. The results of the Intergroup (INT) 01236 trial did not demonstrate a survival benefit to dose-escalation to 64.8 Gy compared with 50.4 Gy, but the results of this have been debated as the majority (7/11) of deaths on the high-dose arm of the trial occurred before reaching 50.4 Gy. Therefore, the INT 0123 study does not preclude the possibility of a benefit with dose escalation.
In surgical candidates, questions have centered on the appropriate dose of radiation offering optimal tumor response yet minimizing postsurgical complications to enhance the therapeutic ratio. In light of the CROSS trial,13 lower doses of 41.4 Gy are acceptable in the neoadjuvant CRT setting in patients who are certain to undergo surgical resection. However, in patients unable to complete surgical resection, or for whose surgery candidacy is equivocal, 41.4 Gy may not be an appropriate dose if these patients are ultimately transitioned to definitive chemoradiation. In such circumstances, a preoperative dose of 50.4 Gy with concurrent chemoradiation may be preferable to ensure that an adequate dose of radiation is administered in case surgical resection cannot be completed.
Results from the CROSS trial allude to the increased likelihood of perioperative pulmonary complications from esophagectomy after neoadjuvant treatment. Wang et al evaluated 110 patients with esophageal cancer treated with trimodality therapy who underwent concurrent chemoradiation with cisplatin, 5-FU and 41.4 to 50.4 Gy followed by surgical resection.18 The primary endpoint of pulmonary complications included pneumonia or acute respiratory distress syndrome (ARDS) within 30 days after surgery. Multivariate analysis showed that the volume of lung spared from doses ≥ 5 Gy (V5) was a significant independent factor associated with postoperative pulmonary complications (p = 0.005). Other studies have indicated that a V10 > 40% resulted in a 35% risk of pneumonia or ARDS.19 Additionally, pericarditis has been noted in up to 27% of patients undergoing chemoradiation for esophageal carcinoma, with highest risk noted among patients who received lung V30 > 46% (risk 73% vs. 13% if the V30 is above or below 46%) and mean dose > 26.1 Gy (risk 73% vs. 13% at doses above and below 26.1 Gy).20 Most recently at the 2018 Gastrointestinal American society of Clinical Oncology (GI ASCO) conference, a study from Memorial Sloan Kettering Cancer Center and the University of Colorado found that that the median overall survival with trimodality therapy dropped from 44 months to 24 months for those who had a total lung V20 ≥ 20%.21 These data illustrate the importance of minimizing lung dose in patients who may proceed to surgical resection, and suggest a possible benefit for patients with radiation modalities that may limit lung dose, such as proton beam therapy (PBT).
Similar to the heterogeneity of doses delivered in preoperative CRT trials, contouring practice varies widely. Matzinger et al reported on the EORTC-ROC guidelines for cancers of the gastroesophageal junction (GEJ) in 2009,22 which differ from the more recent U.S. guidelines by Wu et al designed for integration into intensity-modulated radiation therapy (IMRT) delivery.23 Significant variation of practice with respect to contouring elective nodes exists in the available trials. Moreover, tumors of the most common GEJ location show variation in motion with respect to breathing and heartbeat24 as well as gastric filling.25 At this time, there is no consensus on how best to account for such motion, and studies vary widely.
Many studies discussed in this review employed 3DCRT techniques. With 3DCRT, the esophageal cancer is initially treated using an anterior posterior (AP)/ posterior anterior (PA) field arrangement followed by a cone-down volume with oblique fields angled off the spinal cord. While this approach can minimize dose to the spinal cord, radiation exposure to the heart and lungs remains substantial. This tradeoff has sparked considerable research to improve radiation dose distributions using alternative methods such as IMRT or PBT. Chen et al evaluated helical tomotherapy’s ability to spare heart and lung dose compared with 3DCRT in 6 patients with mid-distal esophageal carcinoma receiving 50 Gy to gross disease.26 Dose-volume histogram (DVH) analysis showed significant sparing of the heart and lung with significantly reduced V30 and V45 in both organs. In a propensity score analysis comparing 3DCRT with IMRT, despite imbalances in the arms favoring 3DCRT (IMRT patients had lower FEV1, poorer performance status, and were less likely to undergo induction chemotherapy) there was an overall survival benefit to patients receiving IMRT compared with 3DCRT (Med OS for IMRT 43 months vs. 25 months for 3DCRT).27 The largest retrospective analysis of nonmetastatic esophageal cancer patients (n = 587) undergoing 50.4 Gy IMRT with concurrent chemoradiation either preoperatively or definitively showed a 3-year OS of 51.8% with very low grade 3 toxicity (1.4% radiation pneumonitis, 13% grade 3 esophagitis).28 A meta-analysis of 5 studies comparing IMRT and 3DCRT treatment of esophageal carcinoma concluded that IMRT can improve overall survival in patients, but did not decrease radiation pneumonitis or radiation esophagitis compared with 3DCRT.29
PBT can further reduce normal tissue radiation exposure beyond the capabilities of IMRT and could further reduce cardiopulmonary toxicity in locally advanced esophageal cancer patients, especially those who undergo trimodality therapy. More recently, a dosimetric study of 10 patients planned to a total dose of 50.4 Gy with 3DCRT, IMRT, and PBT showed benefit of PBT and IMRT over 3DCRT. MD Anderson Cancer Center (MDACC) reported on 62 patients treated with passive scatter PBT and concurrent chemotherapy to a median dose of 50.4 cobalt gray equivalent (CGE) and noted a 28% pCR and 50% near CR rate at the time of surgical resection with decreased local recurrence in the preoperative group compared with the definitive RT group, although OS did not differ between the 2 groups.30 A comprehensive review of PBT for esophageal cancer can be found in the accompanying article by Chuong et al.31
Conclusions and Future Directions
In this article we have reviewed the data driving the management of resectable esophageal carcinoma. Preoperative doses of 41.4 to 50.4 Gy are commonly used with concurrent chemotherapy, with surgical resection to follow 4 to 6 weeks after completion of chemoradiation. To minimize postoperative complications including pulmonary and cardiac toxicity, studies involving modern RT approaches including IMRT and PBT are warranted. Several prospective, advanced modality trials are underway: Loma Linda University (NCT01684904), The Mayo Clinic (NCT02452021), University of Pennsylvania (NCT02213497), and MDACC (NCT01512589). The MDACC study will compare protons and IMRT, while the remainder focus on proton therapy alone. Prospective data from these trials will help clarify future directions in managing resectable locally advanced esophageal carcinoma.
References
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7-30. doi:10.3322/caac.21442.
- Earlam R, Cunha-Melo JR. Oesophageal squamous cell carcinoma: I. A critical review of surgery. Br J Surg. 1980;67(6):381-390. http://www.ncbi.nlm.nih.gov/pubmed/6155968. Accessed May 23, 2018.
- Herskovic A, Martz K, Al-Sarraf M, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med. 1992;326(24): 1593-1598. doi:10.1056/NEJM199206113262403.
- Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA. 1999;281(17):1623-1627. doi:10.1001/jama.281.17.1623.
- Stahl M, Stuschke M, Lehmann N, et al. Chemoradiation with and without surgery in patients with locally advanced squamous cell carcinoma of the esophagus. J Clin Oncol. 2005;23(10):2310-2317. doi:10.1200/JCO.2005.00.034.
- Minsky BD, Pajak TF, Ginsberg RJ, et al. INT 0123 (Radiation Therapy Oncology Group 94-05) phase III trial of combined-modality therapy for esophageal cancer: high-dose versus standard-dose radiation therapy. J Clin Oncol. 2002;20(5):1167-1174. doi:10.1200/JCO.20.5.1167.
- Bedenne L, Michel P, Bouche O, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol. 2007;25(10):1160-1168. doi:10.1200/JCO.2005.04.7118.
- Bosset J-F, Gignoux M, Triboulet J-P, et al. Chemoradiotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N Engl J Med. 1997;337(3):161-167. doi:10.1056/NEJM199707173370304.
- Walsh TN, Noonan N, Hollywood D, et al. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med. 1996;335(7):462-467. doi:10.1056/NEJM199608153350702.
- Urba SG, Orringer MB, Turrisi A, et al. Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol. 2001;19(2):305-313. doi:10.1200/JCO.2001.19.2.305.
- Burmeister B, Smithers M, Gebski V, et al. Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: a randomised controlled phase III trial. Lancet Oncol. 2005;6(9):659-668. doi:10.1016/S1470-2045(05)70288-6.
- Tepper J, Krasna MJ, Niedzwiecki D, et al. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol. 2008;26(7):1086-1092. doi:10.1200/JCO.2007.12.9593.
- van Hagen P, Hulshof MCCM, van Lanschot JJB, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074-2084. doi:10.1056/NEJMoa1112088.
- Best LM, Mughal M, Gurusamy KS. Non-surgical versus surgical treatment for oesophageal cancer. Cochrane Database Syst Rev. 2016;2016(3):CD011498. doi:10.1002/14651858.CD011498.pub2.
- Gebski V, Burmeister B, Smithers BM, et al. Survival benefits from neoadjuvant chemoradiotherapy or chemotherapy in oesophageal carcinoma: a meta-analysis. Lancet Oncol. 2007;8(3):226-234. doi:10.1016/S1470-2045(07)70039-6.
- Shridhar R, Almhanna K, Meredith KL, et al. Radiation therapy and esophageal cancer. Cancer Control. 2013;20(2):97-110. doi:10.1177/107327481302000203.
- Crehange G, Maingon P, Peignaux K, et al. Phase III trial of protracted compared with split-course chemoradiation for esophageal carcinoma: Fédération Francophone de Cancérologie Digestive 9102. J Clin Oncol. 2007;25(31):4895-4901. doi:10.1200/JCO.2007.12.3471.
- Wang SL, Liao Z, Vaporciyan AA, et al. Investigation of clinical and dosimetric factors associated with postoperative pulmonary complications in esophageal cancer patients treated with concurrent chemoradiotherapy followed by surgery. Int J Radiat Oncol Biol Phys. 2006;64(3):692-699. doi:10.1016/j.ijrobp.2005.08.002.
- Lee HK, Vaporciyan AA, Cox JD, et al. Postoperative pulmonary complications after preoperative chemoradiation for esophageal carcinoma: Correlation with pulmonary dose-volume histogram parameters. Int J Radiat Oncol Biol Phys. 2003;57(5):1317-1322. doi:10.1016/S0360-3016(03)01373-7.
- Wei X, Liu HH, Tucker SL, et al. Risk factors for pericardial effusion in inoperable esophageal cancer patients treated with definitive chemoradiation therapy. Int J Radiat Oncol Biol Phys. 2008;70(3):707-714. doi:10.1016/j.ijrobp.2007.10.056.
- Oh P, Zhang M, Brady P, et al. Impact of lung and heart dose on survival after radiotherapy for esophageal cancer. J Clin Oncol. 2018;36(suppl 4S; abstr 3). https://meetinglibrary.asco.org/record/156719/abstract. Accessed May 21, 2018.
- Matzinger O, Gerber E, Bernstein Z, et al. EORTC-ROG expert opinion: radiotherapy volume and treatment guidelines for neoadjuvant radiation of adenocarcinomas of the gastroesophageal junction and the stomach. Radiother Oncol. 2009;92(2):164-175. doi:10.1016/j.radonc.2009.03.018.
- Wu AJ, Bosch WR, Chang DT, et al. Expert consensus contouring guidelines for intensity modulated radiation therapy in esophageal and gastroesophageal junction cancer. Int J Radiat Oncol Biol Phys. 2015;92(4):911-920. doi:10.1016/j.ijrobp.2015.03.030.
- Zhao K, Liao Z, Bucci MK, et al. Evaluation of respiratory-induced target motion for esophageal tumors at the gastroesophageal junction. Radiother Oncol. 2007;84(3):283-289. doi:10.1016/J.RADONC.2007.07.008.
- Bouchard M, McAleer MF, Starkschall G. Impact of gastric filling on radiation dose delivered to gastroesophageal junction tumors. Int J Radiat Oncol. 2010;77(1):292-300. doi:10.1016/j.ijrobp.2009.08.026.
- Chen YJ, Liu A, Han C, et al. Helical tomotherapy for radiotherapy in esophageal cancer: a preferred plan with better conformal target coverage and more homogeneous dose distribution. Med Dosim. 2007;32(3):166-171. doi:10.1016/j.meddos.2006.12.003.
- Lin SH, Wang L, Myles B, et al. Propensity score-based comparison of long-term outcomes with 3-dimensional conformal radiotherapy vs intensity-modulated radiotherapy for esophageal cancer. Int J Radiat Oncol Biol Phys. 2012;84(5):1078-1085. doi:10.1016/j.ijrobp.2012.02.015.
- Shi A, Liao Z, Allen PK, et al. Long-term survival and toxicity outcomes of intensity modulated radiation therapy for the treatment of esophageal cancer: a large single-institutional cohort study. Adv Radiat Oncol. 2017;2(3):316-324. doi:10.1016/j.adro.2017.04.002.
- Xu D, Li G, Li H, Jia F. Comparison of IMRT versus 3D-CRT in the treatment of esophagus cancer: a systematic review and meta-analysis. Medicine (Baltimore, MD). 2017;96(31):e7685. doi:10.1097/MD.0000000000007685.
- Lin SH, Komaki R, Liao Z, et al. Proton beam therapy and concurrent chemotherapy for esophageal cancer. Int J Radiat Oncol Biol Phys. 2012;83(3):e345-51. doi:10.1016/j.ijrobp.2012.01.003.
- Chuong MD, Badiyan S, Hall M, Apisarnthanarx S. Improving the therapeutic index for nonoperable esophageal cancer patients with modern radiation technologies. Appl Radiat Oncol. 2018;7(3):8-14.
Citation
RR R, A K, E N. Controversies in the preoperative radiotherapeutic management of resectable esophageal cancer. Appl Radiat Oncol. 2018;(3):15-20.
September 22, 2018