Leading a Radiation Medicine Department from the Epicenter of the COVID-19 Pandemic in the United States
Images


SA-CME credits are available for this article here.
SARS-CoV-2, or the novel coronavirus, has spread rapidly throughout the world in the early months of 2020, with 2,432,092 confirmed cases worldwide of COVID-19, the disease caused by SARS-CoV-2, and 166,794 deaths as of April 20, 2020.1 The consequent strain on medical resources has been immense. The US overtook China on March 27, 2020, to have the highest number of confirmed cases and on April 17, 2020, the resource utilization estimated national shortage of hospital beds was 5,403, and intensive care unit (ICU) beds was 8,854.1,2 In New York State, with by far the highest COVID-19 burden in the US, those figures were 7,237 hospital beds and 6,175 ICU beds, respectively, on April 9, 2020, the date of peak statewide resource utilization.2 This crisis will likely be the defining event of our generation similar to the world wars in the early and mid-1900s, and how it unfolds over the ensuing months to years remains unclear, with an economic and health impact worldwide yet to be fully recognized.3 The acute redeployment of health care resources toward COVID-19 has had an immediate impact across the entire health care continuum and, in particular, to the treatment of cancer. The broader macro-impact on health outcomes from heart disease to cancer is not likely to be known for months and years to come.
Early Impact of COVID-19 on New York, Northwell Health, and Oncology Population
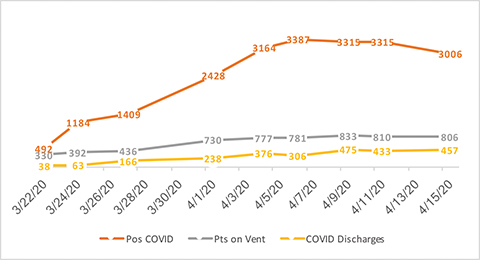
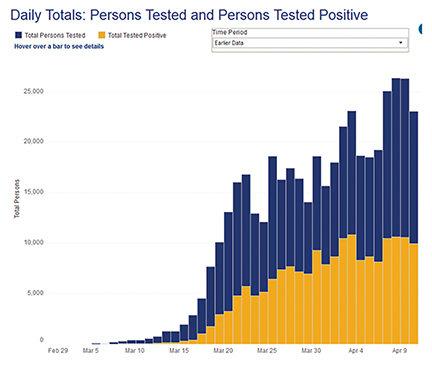
On March 11, 2020, when COVID-19 was officially declared a pandemic by the World Health Organization, there were 56 confirmed cases of COVID-19 in New York State. Shortly after on March 22, New York State closed nonessential businesses and issued a stay-at-home order. As of this writing, there have been 232,782 cases within the Northwell Health geographic area of New York and its suburbs, with 14,137 deaths.4 Since the second week of March 2020, the entire focus of our health system, with 23 hospitals and more than 72,000 employees, has been to stand up more than 1,200 additional inpatient beds and to rebuild and configure spaces in our current buildings for inpatient and ICU care. Auditoriums have been ripped apart. Endoscopy, post-anesthesia care units (PACUs), step-down units and more have been converted into ICUs. Beginning the last week of March, operating rooms (OR) were closed for elective cases except for medical emergencies, with an OR volume normally exceeding 1,000 cases per day reduced to about 80 or less. The ICUs quickly reached capacity with a continued census of more than 800 patients on a ventilator. The burden on the Northwell system (Figure 1) is approximately in line with statewide case and mortality trends (Figure 2).4 It appears that we have hit the peak on hospitalizations with, as of this writing, 3 days of a positive trend where discharges marginally outnumber admissions. Still, the long lengths of stay associated with COVID-19 will require continued redeployment of physicians, nurses, technologists and others to help cover the volume of illness.
The impact on cancer services has been dramatic. The ability to perform surgery, biopsies, and procedures, and offer other ancillary clinical and supportive services has been significantly impacted. We have taken numerous proactive steps to prepare for COVID-19 and implement policies over the past 7 weeks (as of this writing). The purpose of this review article is to outline how the department of radiation medicine has managed the COVID-19 crisis to date.
Impact on Our Radiation Medicine Department
The public health crisis sketched above has had a major downstream impact on medical services not immediately related to its mitigation, including our Radiation Medicine Department. The Department of Radiation Medicine of the Northwell Health Cancer Institute comprises 9 radiation oncology clinics across 6 of the 9 downstate New York counties and provides cancer care to patients throughout this regional area. In the immediate prelude to the pandemic, the department’s daily census on average consisted of 270 patients receiving external-beam radiation, 6 to 10 receiving stereotactic radiosurgery (SRS) or stereotactic body radiation therapy (SBRT), 2 receiving Gamma Knife (Elekta), 20 simulations, 18 new-starts, as well as various brachytherapy procedures, and other patient evaluation and management (E/M) visits. As early as the week of March 9, it was becoming apparent that New York would be significantly affected by COVID-19. This “quiet before the storm” was worsened by constant news reports, which distracted from our day-to-day operations. Nevertheless, we had time to plan without fully recognizing the impact within the department and overall.
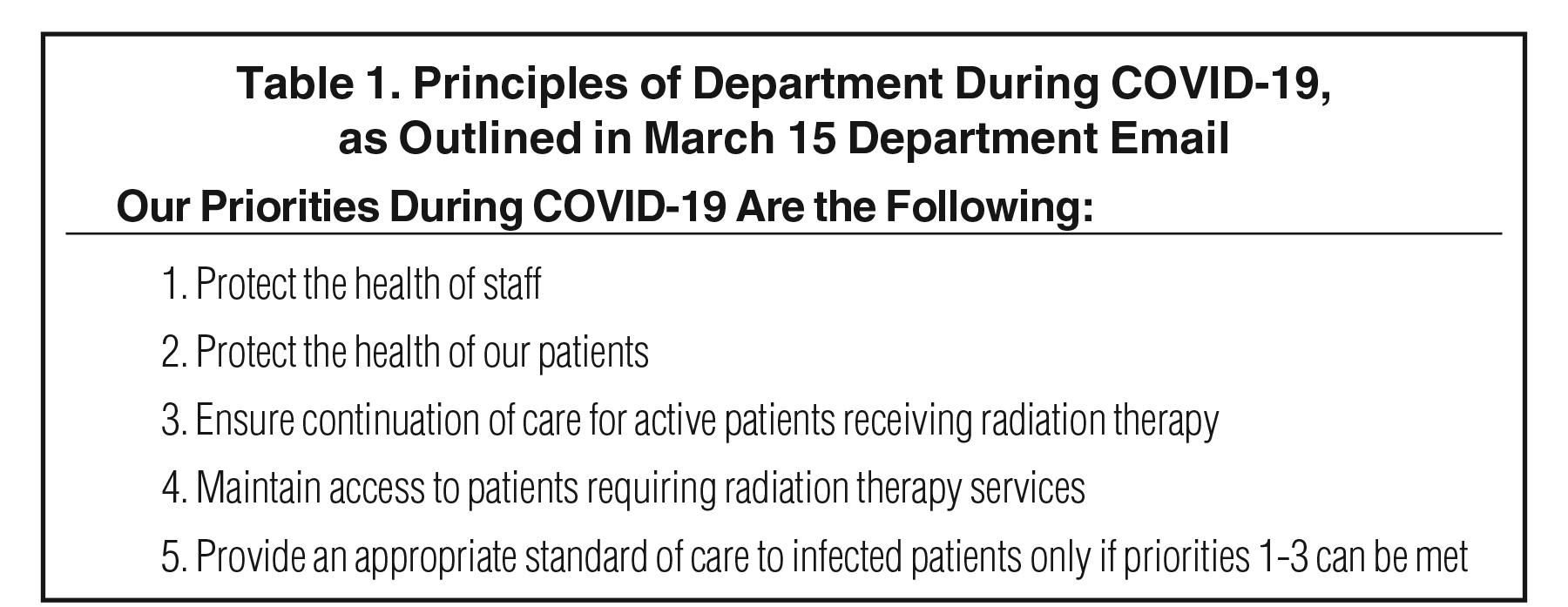
On March 15, an email was sent to our physicians and administrators outlining the over-riding principles (Table 1) and action items needed for safe operations. These principles have served without compromise since.
We also determined that follow-up visits should be curtailed and converted initially to a phone call while telehealth services were being implemented. Additionally, we asked physicians to catalog cases into critical and noncritical categories in case of staffing issues, and to start anticipating cancelled procedures and surgeries.
While we never had an issue obtaining personal protective equipment (PPE) at Northwell, PPE policies evolved during this early phase of the crisis, creating some staff concern and anxiety. Also evolving at this time was the management of staff exposures and patient screening. We started to deploy work-from-home (WFH) orders for some back-office staff, including those performing treatment planning, to reduce personnel volume and thereby lower exposure risk.
Additionally, on March 17, we issued a policy for our residency program to protect residents and minimize their exposure without compromising training. The policy stated that residents would immediately do the following: WFH on their attendings’ academic days and other days when no clinic or hospital visits were scheduled for their respective services; don context-appropriate PPE for all patient encounters; perform contouring, plan review, clinical note writing, and other such work remotely to the extent feasible; and participate in didactic sessions and tumor boards via video chat and/or teleconference. On April 1, we also implemented weekly teleconference check-ins between the residents and program director regarding operational concerns and resident well-being.
Prioritizing Patients for Radiation Start
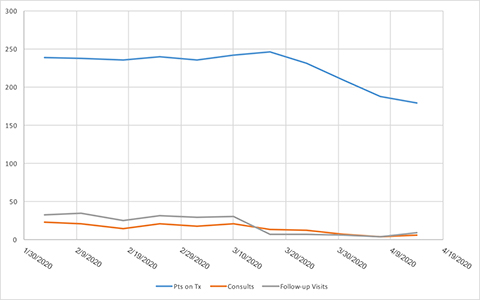
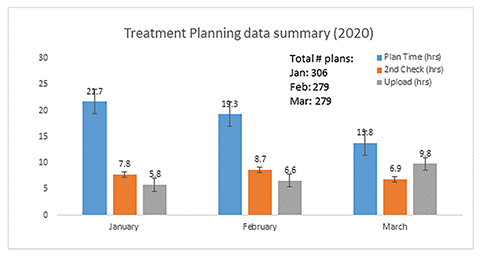
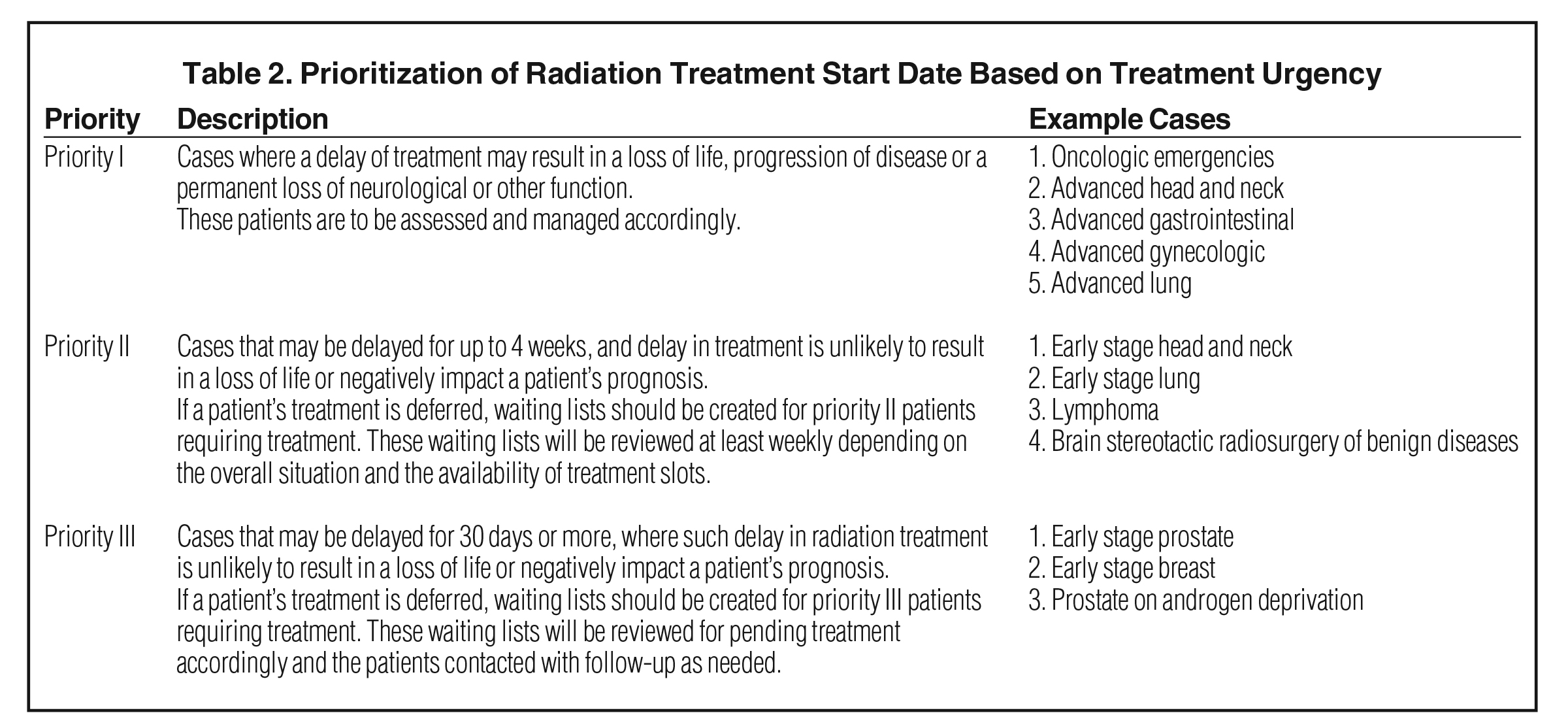
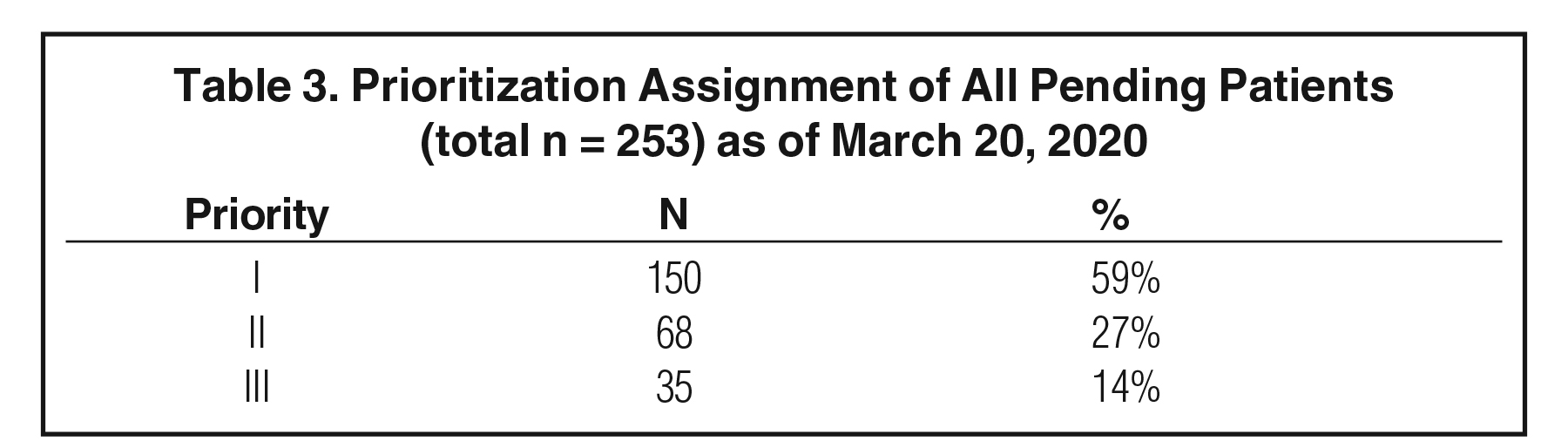
By March 19 a more detailed outline was developed to prioritize patient treatment urgency into three categories (Table 2). At that time, we had 253 patients in the queue between consultation and treatment start. A department-wide video conference was convened on the morning of March 20 where each case was presented and assigned a priority (Table 3). While it was laudable to delay the start of up to 40% of our patients, it was not clear if or how many of the staff would become sick and if we could continue to offer access to current patients. As a result, our on-treatment patient volume did not decompress for another 2 weeks due to lagging attrition (Figure 3). Although we never experienced a reduction in staff, we had developed contingency plans to maintain access and treatment if that had happened.5 Likewise, our physics department smoothly transitioned to WFH, with shorter planning times and slightly longer plan upload times likely due to virtual private network (VPN) connectivity (Figure 4).
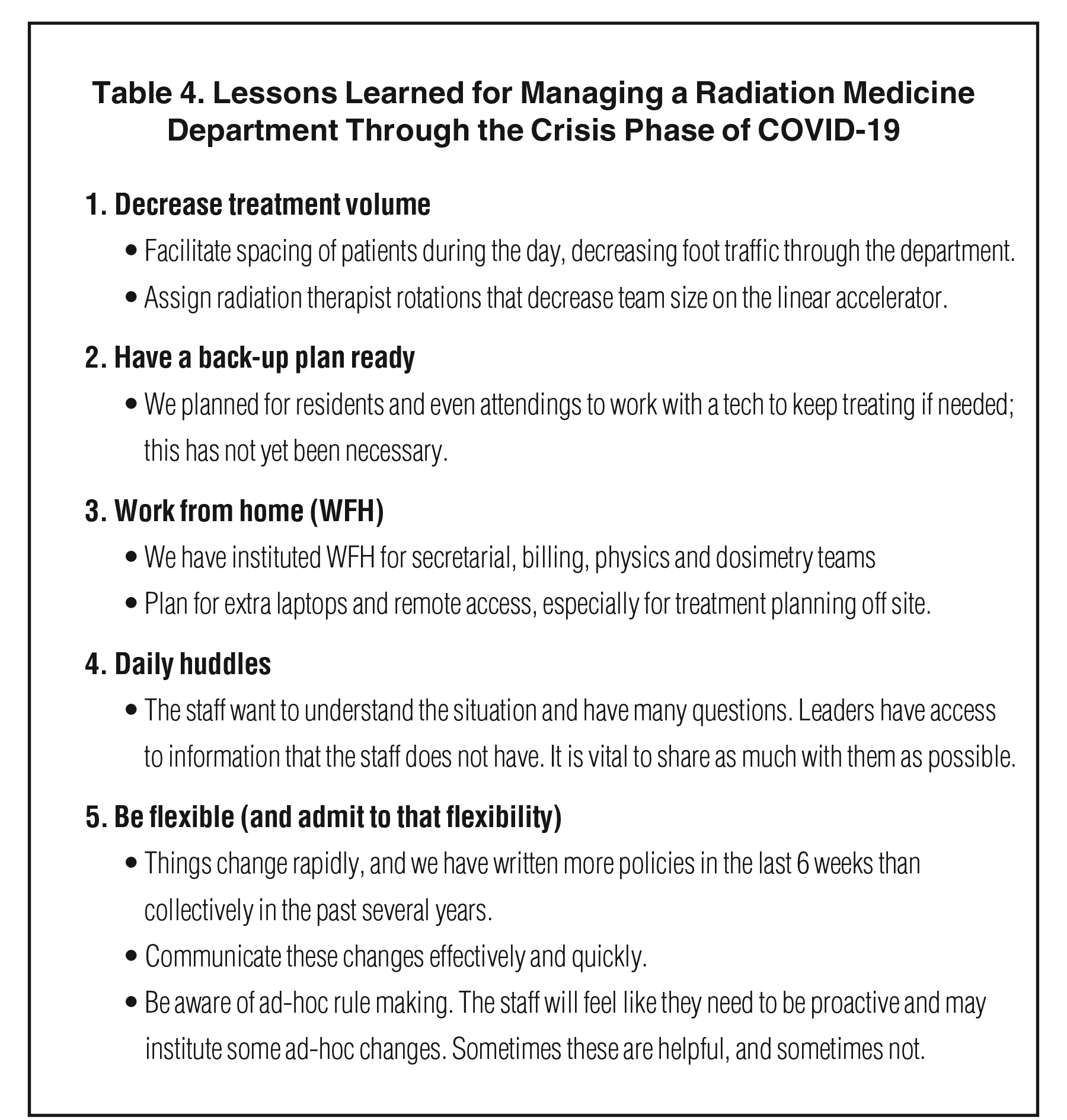
Other actions during the week of March 16-20 included starting a daily administrative operations call, creating a new huddle for on-site staff (at appropriate distance), pre-screening patients before entering our waiting room, converting more than 70% of our E/M visits to telehealth, and managing several staff rule-outs and rule-ins for COVID-19 (Table 4).
Maintaining a Culture of Safety
It is critical in a crisis to maintain departmental rules and policies regarding patient safety. During the COVID-19 crisis, we have made a purposeful decision not to relax safety rules whatsoever and to not allow workarounds, but rather to assess and view these rules as the foundation of providing safe care. Doing so has created a routine and set of expectations that have grounded the staff during the uncertainty of a health crisis unfolding around them. Opportunities to explore modifications of these safety rules provide fresh perspectives toward established policies. However, we have refrained from making such changes in the midst of the crisis, and instead have cataloged feedback from faculty and staff for future discussion, when we are past the acute crisis phase.
Management of SARS-CoV-2 Positivity Among Staff and Patients
The department has had several staff members test positive for SARS-CoV-2 virus. This understandably creates anxiety regarding potential exposures. Fortunately, we have seen relatively little cross infection except at one of our locations early in the crisis where several staff tested positive together. When staff were known to have tested positive for the virus, all patients and staff with whom they had come in contact in the 48 hours prior to falling ill were informed of the exposure. We followed CDC guidelines for health care workers (HCWs) stating that asymptomatic HCWs who had been exposed to a known COVID-19 case should continue working while wearing a surgical mask and undergo twice-daily temperature and symptom reporting. We attribute the low departmental infection rate to Northwell’s early policy requiring clinical staff to wear surgical masks at all times, high staff awareness about infection prevention, and a policy requiring patients to wear masks. In addition, the health system instituted an early policy prohibiting in-person group meetings including teaching conferences and tumor boards. This allowed staff to limit exposure to each other and reduced the need to travel between our outpatient and inpatient sites for nonpatient-care-related activities. Further, we protected patients and staff by requiring patients to undergo telephone screening 24 hours prior to their appointment.
We continue to treat infected patients with full PPE with an approach involving the use of a rear door, limited exposure time, increased physical distance, appropriate donning and doffing of full PPE, and appropriate vault decontamination (Figure 5). The ability to treat a positive patient in their acute phase of COVID-19 and then to have the illness resolve and continue treatment without the need for full PPE and without a break is also very encouraging.
Current Status: Seven Weeks into the Crisis
Our treatment numbers are about 70% of typical volume and it was helpful to arrive here as we initially did not know how staff would be affected. We are calling this our “soft landing.” Now that we are in this position, we can better control new patient flow, with many in the queue assigned a priority level of 2. We continue to space out treatments to decrease foot traffic in the waiting room. Coupled with telehealth, our distancing measures have proven highly successful.
As the crisis in New York remains critical, the issue now is redeploying staff. We have had staff from all departmental areas redeployed to inpatient or ambulatory care. Specifically, several nurse practitioners and physician assistants worked on inpatient COVID units for 2 to 4 weeks at a time. Physicians were also added to a redeployment list, but to date were not needed to staff COVID units. It is not clear if this will remain a short- or long-term policy but to date we have not faced critical staffing issues.
We have also begun screening all patients who enter our departments for symptoms related to COVID-19 and we have discouraged visitors from accompanying patients unless they are a formal caregiver. If screening indicates concerning symptoms, the patient is isolated, formally evaluated by a clinician, and referred for immediate testing in our ambulatory locations. Specific ambulatory offices throughout our health system have now been converted for exclusive use as testing centers.
Another area we are addressing is hospital avoidance for our patients (Table 5). The goal is to keep our active on-treatment patients out of emergency departments and hospitals. Hospitals are no longer a sanctuary site for supportive cancer care, but rather an iatrogenic risk site with limited resources for the cancer patient. We will be doing things differently with regards to pre-, on-, and post-treatment management, and we are hopeful that some of these changes may make a long-term difference.5
Recommendations for Crisis Management
The COVID-19 pandemic represents a challenge to medical practice that is unprecedented in living memory. As other authors have noted, oncology patients face a uniquely precarious situation during this crisis: They are likely to be at elevated risk of severe complications of SARS-Cov-2 infection on the basis of age and pathology alone, and are at further heightened risk of exposure as a consequence of the oncologic interventions intended to prolong life and/or improve quality of life. Patients and their providers must negotiate a Morton’s fork between foregoing oncologic care and potentially succumbing prematurely to cancer, or pressing forward with that care and risk succumbing to COVID-19 complications.6,7
Moving from the individual doctor- and-patient approach to a system-wide view, oncology departments must take stock of where they find themselves in the framework proposed by Schrag et al: in preparatory, acute, or crisis phases of the pandemic.7 As of this writing, the majority of the US is in a preparatory phase (intact system with a surplus of manpower and equipment) or acute phase (a system under strain with reduced capacity that can still meet its needs by strategic resource allocations). New York and much of the Northeast, Louisiana, and Michigan are in a crisis phase: a system overwhelmed and facing shortages. It is crucial to marshal resources and prepare staff during the preparatory and acute phases to withstand the crisis phase and minimize the impact on care, to lay plans in advance for a transition out of crisis phase, and indeed to lay preparations for the possibility of cycling between these phases given the possibility of subsequent spikes of infection resulting from causes beyond health care systems’ control.3
The challenge of oncology care during this crisis is further exacerbated by the loss of oncologic surgeries due to the lack of OR resources and the need to preserve hospital space for COVID-19 patients. This impact also includes the limitation or curtailment of brachytherapy procedures leading us to move away from an accepted standard of care in many instances. From a radiation oncology perspective, there has been a push to shorten treatment courses by implementing hypofractionated options to replace protracted conventionally fractionated radiation therapy. While some of these shorter fractionation schedules have evidence-based outcomes, many alternative treatment schedules have not undergone the same breadth of data collection and analysis. In addition, many physicians may find themselves uncomfortable with these regimens and unable to counsel patients appropriately on the expected short- and long-term effects. Examples include adoption of single-fraction regimens in settings ranging from curative-intent thoracic SBRT to palliative radiation therapy in oncologic emergencies, instead of the multifraction approaches that would be favored under ordinary circumstances.8.9 Likewise, from a medical oncology perspective, re-evaluation of oral over intravenous chemotherapy and keeping patients out of infusion facilities remains circumspect with regard to equivalent or non-inferior outcomes.7
Oncology, by its nature, is a multidisciplinary enterprise and oncologic care is optimized by communication and coordination of therapy between its various clinical branches and in collaboration across health systems. It is encouraging, in this context, to see the swift adoption across many practices nationally and internationally of similar policies to limit clinical volumes and treatment times, while maintaining social distancing as well as the morale and health of providers and ancillary staff.7-12
Conclusion
It is undeniable that delays in delivering oncologic care secondary to the scarcity of resources and need for strict social distancing will impact patient outcomes. The degree of that impact, and in which settings it is most significant, will be an urgent subject of future study and analysis. We have outlined here our systematic approach to mitigate that impact to whatever extent is feasible and safe in the interim. Our mission in this crisis is to continue to provide exemplary oncologic care while contributing to the public health of our community — perhaps the most severely and acutely affected of any in the world – and we are unwavering in our commitment to do so.
References
- Johns Hopkins Coronavirus Resource Center. Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. Accessed April 18, 2020. https://coronavirus.jhu.edu/us-map
- Institute for Health Metrics and Evaluation. COVID-19 Projections, Institute for Health Metrics and Evaluation (IHME) at the University of Washington. Accessed April 18, 2020. https://covid19.healthdata.org/
- Kissler SM, Tedijanto C, Goldstein E, Grad YH, Lipsitch M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science. April 14, 2020.
- New York State Department of Health. NYSDOH COVID-19 Tracker. Accessed April 18, 2020. https://covid19tracker.health.ny.gov/views/NYS-COVID19-Tracker/NYSDOHCOVID-19Tracker-DailyTracker?%3Aembed=yes&%3Atoolbar=no&%3Atabs=n
- Chen W, Teckie S, Somerstein G, Adair N, Potters L. Guidelines to reduce hospitalization rates for patients receiving curative-intent radiation therapy during the COVID-19 pandemic: report from a multicenter New York area institution. Adv Rad Onc, April 2020. https://www.astro.org/ASTRO/media/ASTRO/Daily%20Practice/PDFs/COVID-Chen-et-al(ADRO).pdf
- Thomson DJ, Palma D, Guckenberger M, et al. Practice recommendations for risk-adapted head and neck cancer radiotherapy during the COVID-19 pandemic: an ASTRO-ESTRO Consensus Statement. Int J Radiat Oncol Biol Phys. Apr 14;S0360-3016(20)31034-8. https://doi.org/10.1016/j.ijrobp.2020.04.016
- Schrag D, Hershman DL, Basch E. Oncology practice during the COVID-19 pandemic. J Am Med Assoc. April 13, 2020. https://doi.org/10.1001/jama.2020.6236
- Wu, Abraham, Rimmer, Andreas, et al. Thoracic radiation therapy during COVID-19: provisional guidelines from a comprehensive cancer center within a pandemic epicenter. Adv Rad Onc. April 2020. https://www.astro.org/ASTRO/media/ASTRO/Daily%20Practice/PDFs/COVID-Wu-et-al(ADRO).pdf
- Yaerramilli D, Xu AJ, Gillespie EF, et al. Palliative radiotherapy for oncologic emergencies in the setting of COVID-19: approaches to balancing risks and benefits. Adv Rad Onc. April 8, 2020. https://doi.org/10.1016/j.adro.2020.04.001
- Noticewala S, Koong A, Bloom EC, et al. Strategies to flatten the curve during the COVID-19 pandemic in radiation oncology: experience from a large tertiary cancer center. Adv Rad Onc. April 2020. https://www.astro.org/ASTRO/media/ASTRO/Daily%20Practice/PDFs/COVID-Noticewala-et-al(ADRO).pdf
- Rathod S, Dubey A, Chowdhury A, Bashir B, Koul R. A call for new 4R’s based radiation oncology model in COVID-19 Pandemic. Adv Rad Onc. April 2020. https://www.astro.org/ASTRO/media/ASTRO/Daily%20Practice/PDFs/COVID-Rathod-et-al(ADRO).pdf
- Simcock R, Thomas TV, Christopher E, et al. COVID-19: Global radiation oncology’s targeted response for pandemic preparedness. Clin Transl Radiat Oncol. 2020 Mar 24;55-68. https://doi.org/10.1016/j.ctro.2020.03.009.
- Common Terminology Criteria for Adverse Events (CTCAE). 2017:147.
- Ajani JA, Winter KA, Gunderson LL, et al. Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. JAMA. 2008;299(16):1914-1921. doi:10.1001/jama.299.16.1914
- Mitra D, Hong TS, Horick N, et al. Long-term outcomes and toxicities of a large cohort of anal cancer patients treated with dose-painted IMRT per RTOG 0529. Adv Rad Onc. 2017;2(2):110-117. doi:10.1016/j.adro.2017.01.009
- National Comprehensive Cancer Network. Rectal Cancer (Version 2.2020). Accessed May 8, 2020. https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf
- National Comprehensive Cancer Network. Esophageal and Esophagogastric Junction Cancers (Version 1.2020). Accessed May 8, 2020. https://www.nccn.org/professionals/physician_gls/pdf/esophageal.pdf
- Al-Batran S-E, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957. doi:10.1016/S0140-6736(18)32557-1
Citation
Koffler D, Teckie S, Potters L. Leading a Radiation Medicine Department from the Epicenter of the COVID-19 Pandemic in the United States. Appl Rad Oncol. 2020;(2):15-22.
June 22, 2020

Latest Review Articles
- A Narrative Review on Radiation Oncology Physician Well-Being in the United States
- A Novel Framework to Define and Prognosticate Visual Outcomes Following Fractionated Radiation Therapy for Optic Nerve Sheath
- A Practical Method to Prolong Expiratory Breath Holds for Abdominal Stereotactic Body Radiation Therapy
- Radiation Therapy-Induced Toxicity in a Breast Cancer Patient With Variance of Unknown Significance in the Ataxia Telangiectasia
- Late Effects of Pelvic Radiation Therapy in the Female Patient: A Comprehensive Review